

Secondary Cervicothoracic Scoliosis in Congenital Muscular Torticollis
- PMID: 31475057
- PMCID: PMC6695322
- DOI: 10.4055/cios.2019.11.3.344
Secondary Cervicothoracic Scoliosis in Congenital Muscular Torticollis
Abstract
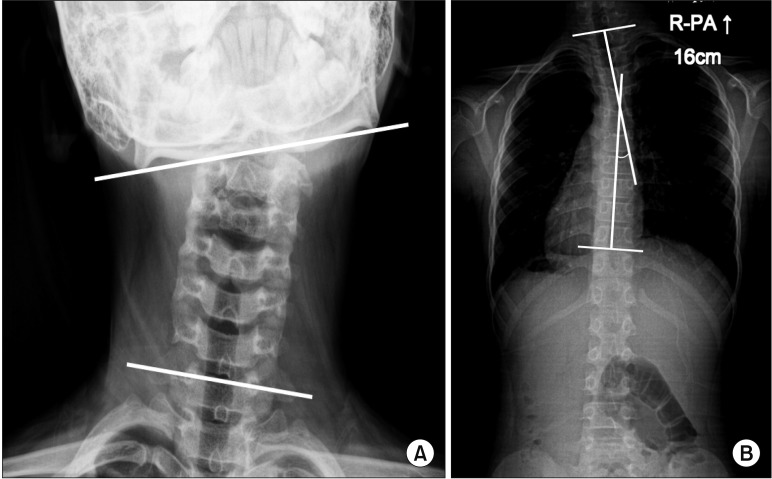
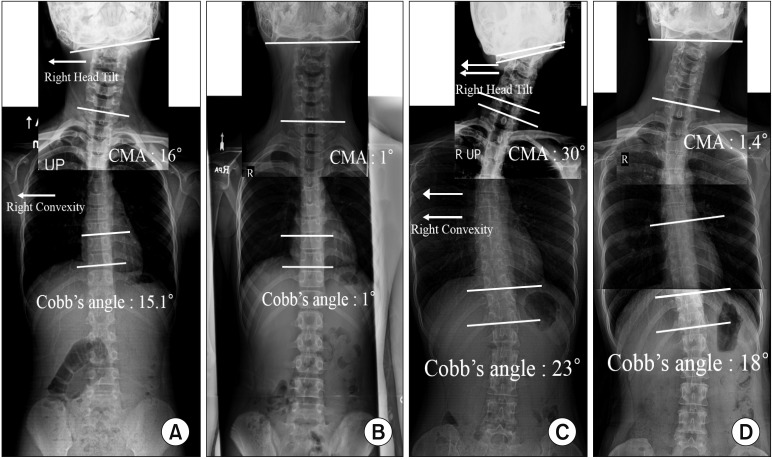
Background: Although secondary cervicothoracic scoliosis frequently occurs in patients with congenital muscular torticollis (CMT), the relationship between scoliosis and CMT has not been evaluated. This study aims to evaluate the effects of surgical release of sternocleidomastoid (SCM) muscle on secondary cervicothoracic scoliosis in patients with CMT and determine factors affecting the improvement of scoliosis after surgical release of SCM muscle.
Methods: Eighty-seven of the 106 patients, confirmed as having secondary cervicothoracic scoliosis with CMT with a minimum 1-year follow-up, were included in this study. Preoperative and last follow-up radiologic outcomes were assessed for the cervicomandibular angle (CMA), Cobb angle of the cervicothoracic scoliosis, and direction of convexity in the scoliosis curve. Patients were divided into two groups to assess the improvement of Cobb angle according to residual growth potential; age ≤ 15 years and > 15 years. The improvement of Cobb angle after surgical release was compared in the two groups. Correlation analysis and multivariable regression analysis were performed to determine the factors affecting the improvement of scoliosis.
Results: All the radiologic parameters, such as the Cobb angle and CMA, improved significantly after surgical release (p < 0.001). The improvement of Cobb angle was significantly higher in age ≤ 15 years than in age > 15 years (p < 0.001). The improvement of Cobb angle was significantly correlated with age (r = -0.474, p < 0.001) and the preoperative Cobb angle (r = 0.221, p = 0.036). In multivariable regression analysis, age and preoperative Cobb angle were shown to be predisposing factors affecting the improvement of scoliosis.
Conclusions: The results showed that SCM release can be a beneficial treatment for secondary cervicothoracic scoliosis. The improvement of scoliosis was greater when the SCM release was performed before the patient reached the end of growth.
Keywords: Cervicomandibular angle; Cobb angle; Congenital muscular torticollis; Secondary scoliosis; Sternocleidomastoid release.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Ta JH, Krishnan M. Management of congenital muscular torticollis in a child: a case report and review. Int J Pediatr Otorhinolaryngol. 2012;76(11):1543–1546. - PubMed
-
- Hussein MA, Yun IS, Park H, Kim YO. Cervical spine deformity in long-standing, untreated congenital muscular torticollis. J Craniofac Surg. 2017;28(1):46–50. - PubMed
-
- Lee JK, Moon HJ, Park MS, Yoo WJ, Choi IH, Cho TJ. Change of craniofacial deformity after sternocleidomastoid muscle release in pediatric patients with congenital muscular torticollis. J Bone Joint Surg Am. 2012;94(13):e93. - PubMed
-
- Seo SJ, Kim JH, Joh YH, et al. Change of facial asymmetry in patients with congenital muscular torticollis after surgical release. J Craniofac Surg. 2016;27(1):64–69. - PubMed
-
- Seo SJ, Yim SY, Lee IJ, et al. Is craniofacial asymmetry progressive in untreated congenital muscular torticollis? Plast Reconstr Surg. 2013;132(2):407–413. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
