

Cancer-Specific Thresholds Adjust for Whole Exome Sequencing-based Tumor Mutational Burden Distribution
- PMID: 31475242
- PMCID: PMC6716608
- DOI: 10.1200/PO.18.00400
Cancer-Specific Thresholds Adjust for Whole Exome Sequencing-based Tumor Mutational Burden Distribution
Abstract
Purpose: To understand the clinical context of tumor mutational burden (TMB) when comparing a pan-cancer threshold and a cancer-specific threshold.
Materials and methods: Using whole exome sequencing (WES) data from primary tumors in The Cancer Genome Atlas (TCGA) (n=3,534) and advanced/metastatic tumors from Weill Cornell Medicine (WCM Advanced) (n=696), TMB status was determined using a pan-cancer and cancer-specific threshold. Survival curves, number of samples classified as TMB high, and predicted neoantigens were used to evaluate the differences between thresholds.
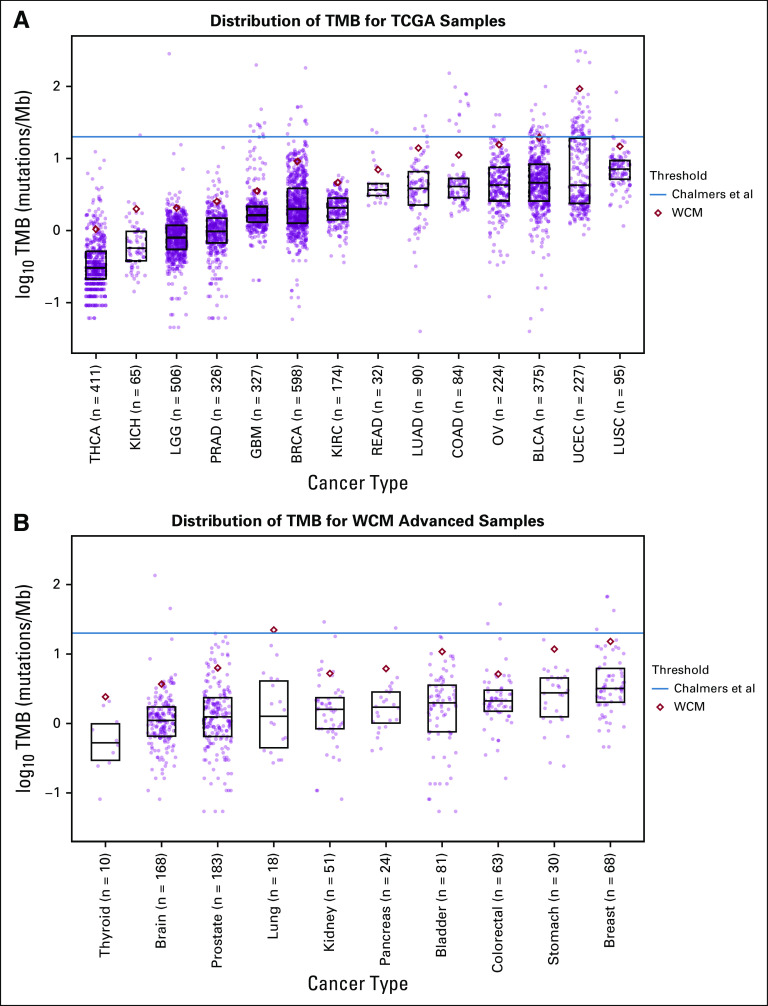
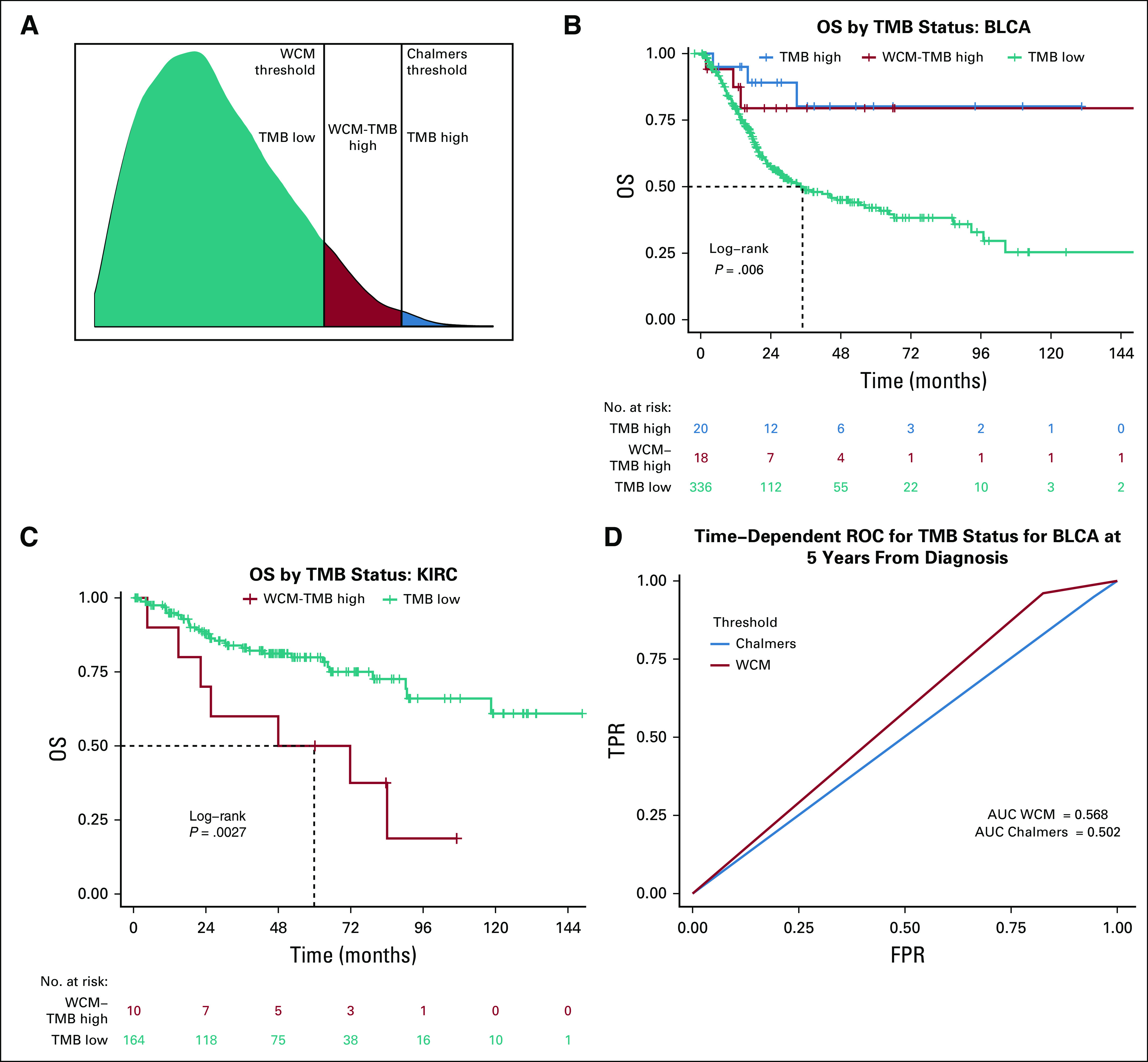
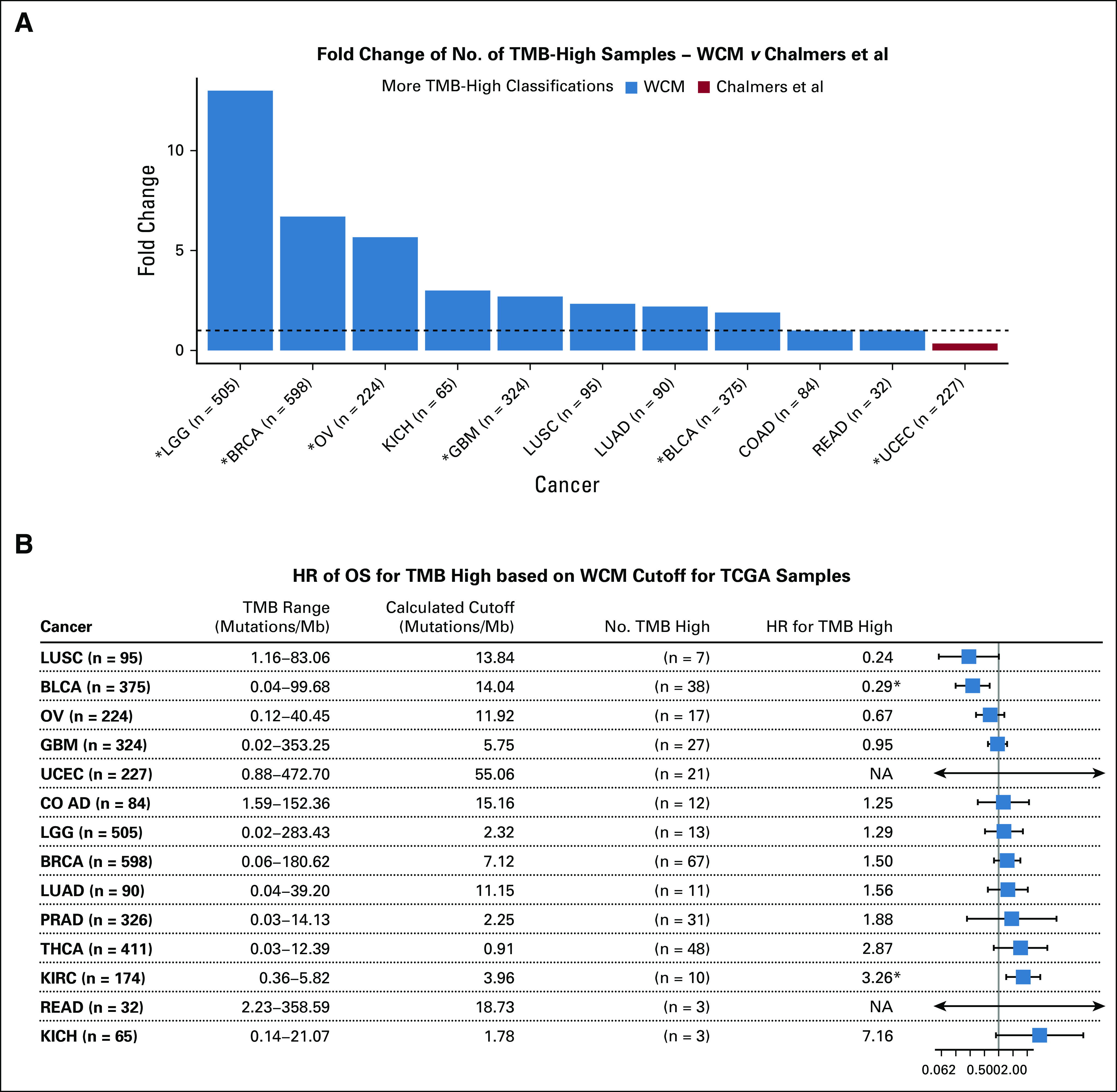
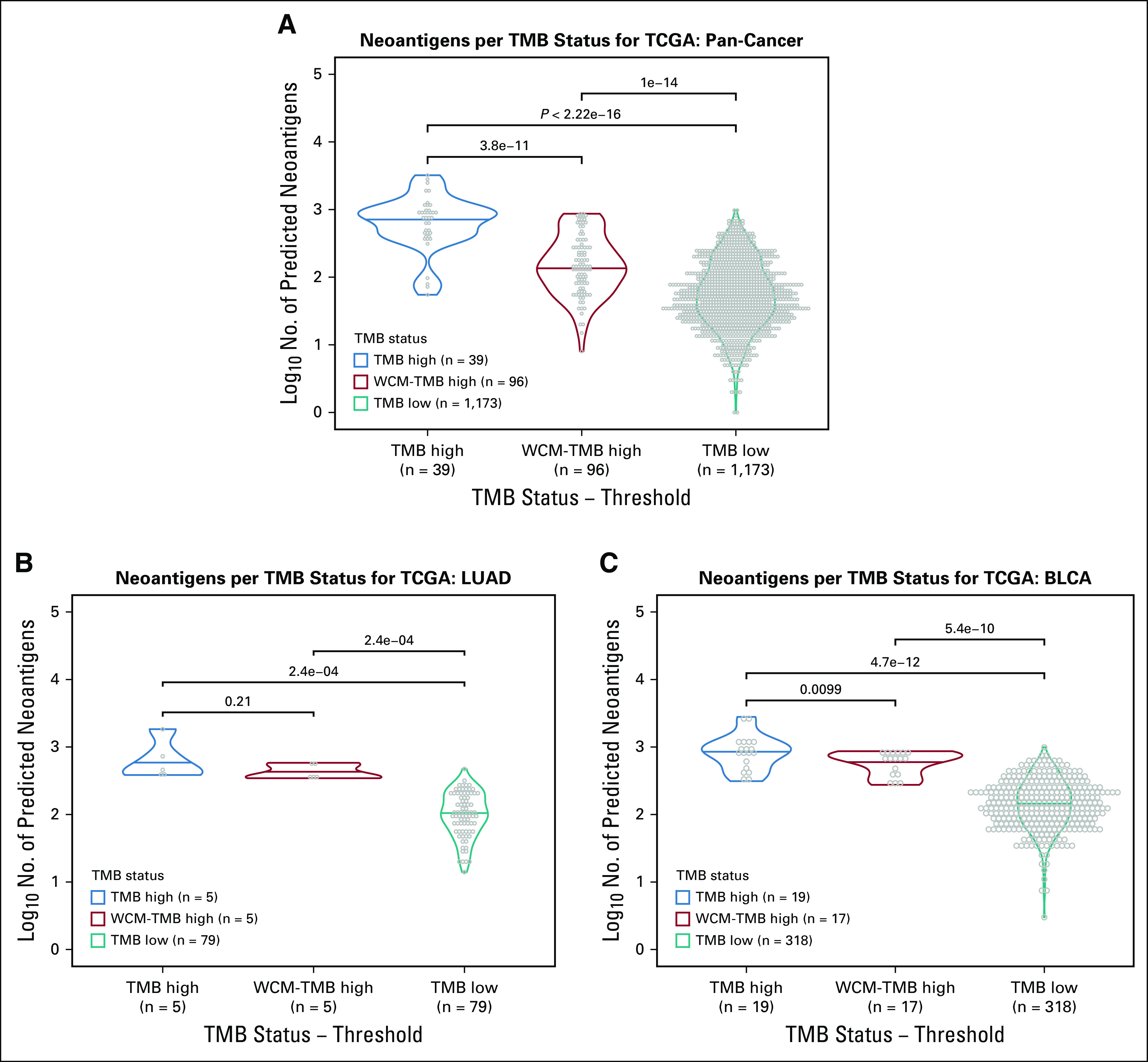
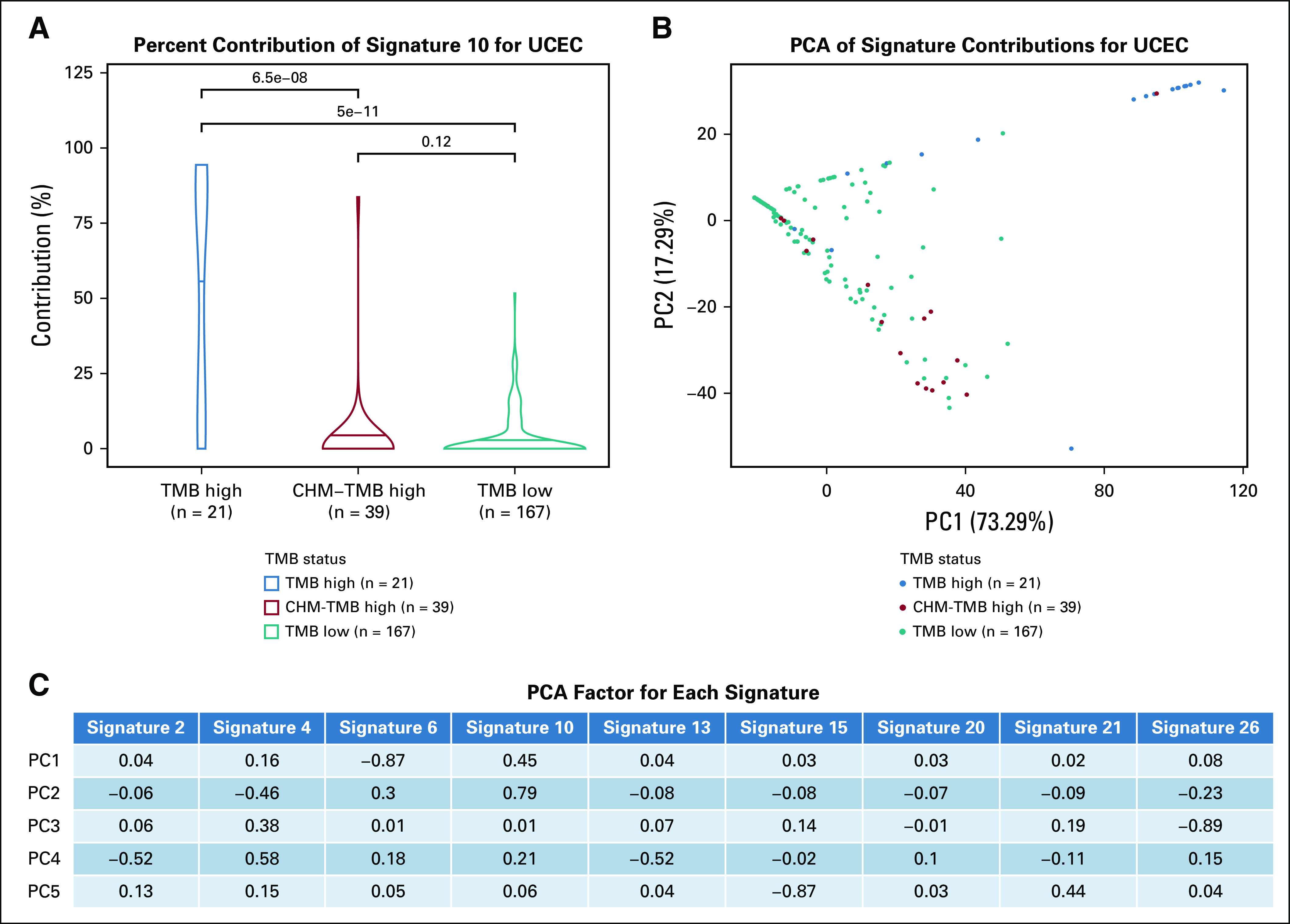
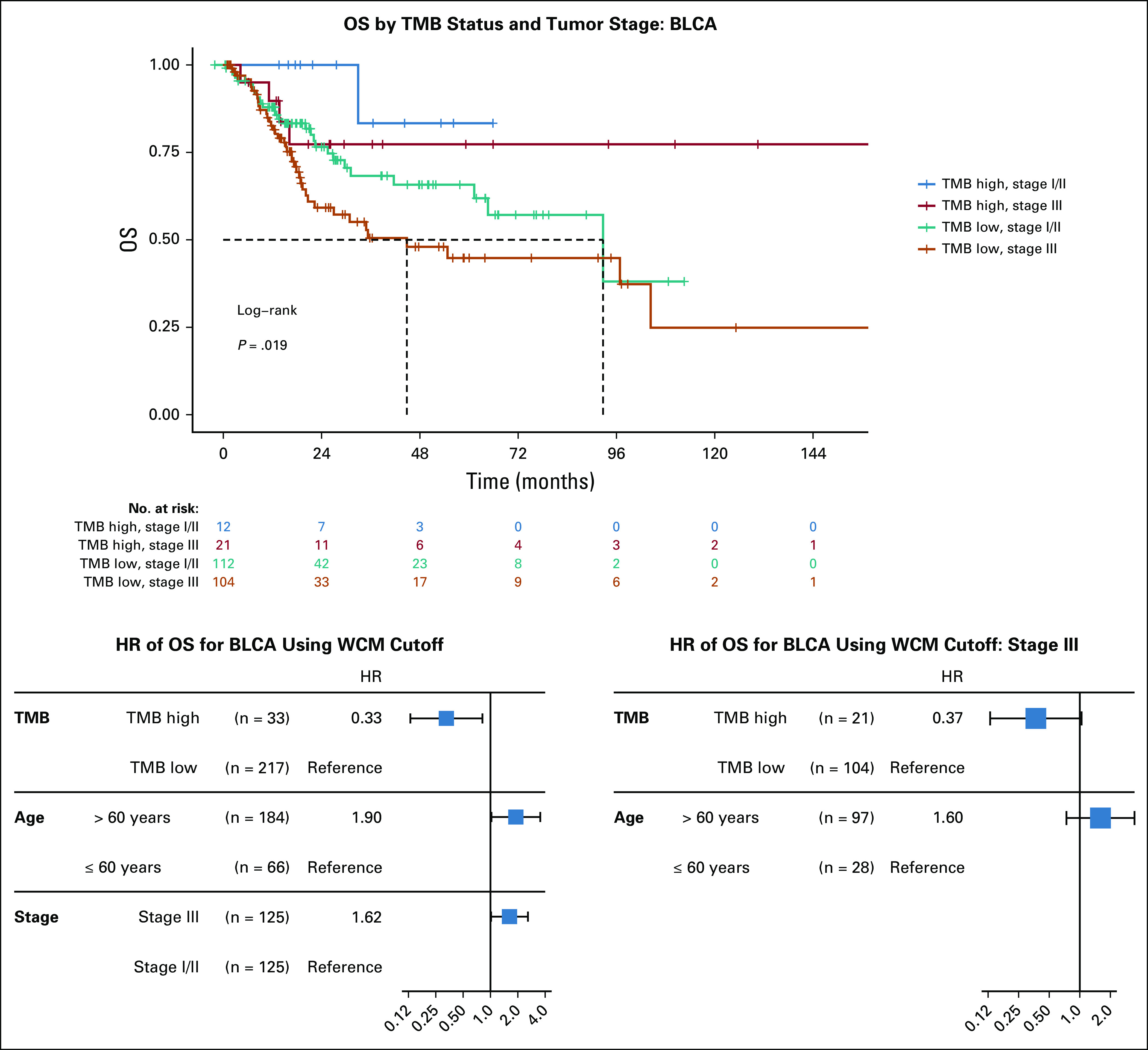
Results: The distribution of TMB varied dramatically between cancer types. A cancer-specific threshold was able to adjust for the different TMB distributions, while the pan-cancer threshold was often too stringent. The dynamic nature of the cancer-specific threshold resulted in more tumors being classified as TMB high compared to the static pan-cancer threshold. Additionally, no significant difference in survival outcomes was found with the cancer-specific threshold compared to the pan-cancer one. Further, the cancer-specific threshold maintains higher predicted neoantigen load for the TMB high samples compared to the TMB low samples, even when the threshold is lower than the pan-cancer threshold.
Conclusion: TMB is relative to the context of cancer type, metastatic state, and disease stage. Compared to a pan-cancer threshold, a cancer-specific threshold classifies more patients as TMB high while maintaining clinical outcomes that were not significantly different. Furthermore, the cancer-specific threshold identifies patients with a high number of predicted neoantigens. Due to the potential impact in cancer patient care, TMB status should be determined in a cancer-specific manner.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Evan M. Fernandez
Himisha Beltran
Bishoy M. Faltas
Juan Miguel Mosquera
David M. Nanus
Brian D. Robinson
Mark A. Rubin
Olivier Elemento
Manish A. Shah
Wei Song
No other potential conflicts of interest were reported.
Figures
References
-
- Tray N, Weber JS, Adams S. Predictive biomarkers for checkpoint immunotherapy: Current status and challenges for clinical application. Cancer Immunol Res. 2018;6:1122–1128. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
