

Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment With Cardiac Structure and Function in Patients With Heart Failure With Reduced Ejection Fraction
- PMID: 31475295
- PMCID: PMC6724151
- DOI: 10.1001/jama.2019.12821
Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment With Cardiac Structure and Function in Patients With Heart Failure With Reduced Ejection Fraction
Abstract
Importance: In patients with heart failure and reduced ejection fraction (HFrEF), treatment with sacubitril-valsartan reduces N-terminal pro-b-type natriuretic peptide (NT-proBNP) concentrations. The effect of sacubitril-valsartan on cardiac remodeling is uncertain.
Objective: To determine whether NT-proBNP changes in patients with HFrEF treated with sacubitril-valsartan correlate with changes in measures of cardiac volume and function.
Design, setting, and participants: Prospective, 12-month, single-group, open-label study of patients with HFrEF enrolled in 78 outpatient sites in the United States. Sacubitril-valsartan was initiated and the dose adjusted. Enrollment commenced on October 25, 2016, and follow-up was completed on October 22, 2018.
Exposures: NT-proBNP concentrations among patients treated with sacubitril-valsartan.
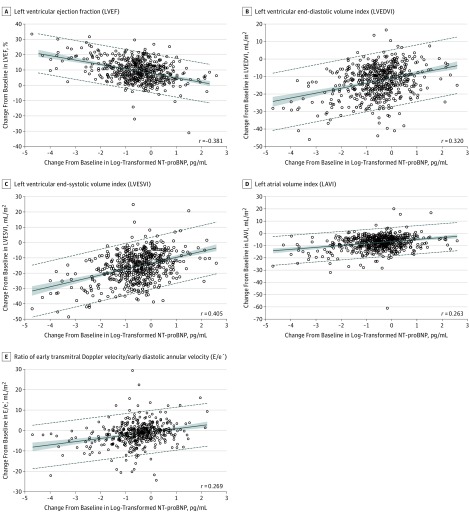
Main outcomes and measures: The primary outcome was the correlation between changes in log2-NT-proBNP concentrations and left ventricular (LV) EF, LV end-diastolic volume index (LVEDVI), LV end-systolic volume index (LVESVI), left atrial volume index (LAVI), and ratio of early transmitral Doppler velocity/early diastolic annular velocity (E/e') at 12 months.
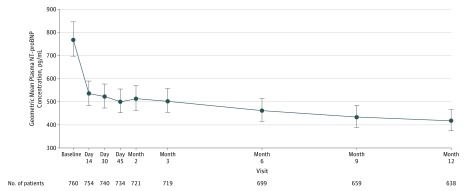
Results: Among 794 patients (mean age, 65.1 years; 226 women [28.5%]; mean LVEF = 28.2%), 654 (82.4%) completed the study. The median NT-proBNP concentration at baseline was 816 pg/mL (interquartile range [IQR], 332-1822) and 455 pg/mL (IQR, 153-1090) at 12 months (difference, P < .001). At 12 months, the change in log2-NT-proBNP concentration was correlated with changes in LVEF (r = -0.381 [IQR, -0.448 to -0.310]; P < .001), LVEDVI (r = 0.320 [IQR, 0.246 to 0.391]; P < .001), LVESVI (r = 0.405 [IQR, 0.335 to 0.470]; P < .001), LAVI (r = 0.263 [IQR, 0.186 to 0.338]; P < .001), and E/e' (r = 0.269 [IQR, 0.182 to 0.353]; P < .001). At 12 months, LVEF increased from 28.2% to 37.8% (difference, 9.4% [95% CI, 8.8% to 9.9%]; P < .001), while LVEDVI decreased from 86.93 to 74.15 mL/m2 (difference, -12.25 mL/m2 [IQR, -12.92 to -11.58]; P < .001) and LVESVI decreased from 61.68 to 45.46 mL/m2 (difference, -15.29 mL/m2 [95% CI, -16.03 to -14.55]; P < .001). LAVI and E/e' ratio also decreased significantly. The most frequent adverse events were hypotension (17.6%), dizziness (16.8%), hyperkalemia (13.2%), and worsening kidney function (12.3%).
Conclusions and relevance: In this exploratory study of patients with HFrEF treated with sacubitril-valsartan, reduction in NT-proBNP concentration was weakly yet significantly correlated with improvements in markers of cardiac volume and function at 12 months. The observed reverse cardiac remodeling may provide a mechanistic explanation for the effects of sacubitril-valsartan in patients with HFrEF.
Trial registration: ClinicalTrials.gov Identifier: NCT02887183.
Conflict of interest statement
Figures
Comment in
-
Mechanisms of sacubitril-valsartan benefit in HFrEF.Nat Rev Cardiol. 2019 Nov;16(11):648. doi: 10.1038/s41569-019-0282-2. Nat Rev Cardiol. 2019. PMID: 31537918 No abstract available.
References
-
- Kramer DG, Trikalinos TA, Kent DM, Antonopoulos GV, Konstam MA, Udelson JE. Quantitative evaluation of drug or device effects on ventricular remodeling as predictors of therapeutic effects on mortality in patients with heart failure and reduced ejection fraction: a meta-analytic approach. J Am Coll Cardiol. 2010;56(5):392-406. doi:10.1016/j.jacc.2010.05.011 - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
