

Association of Metabolic Surgery With Major Adverse Cardiovascular Outcomes in Patients With Type 2 Diabetes and Obesity
- PMID: 31475297
- PMCID: PMC6724187
- DOI: 10.1001/jama.2019.14231
Association of Metabolic Surgery With Major Adverse Cardiovascular Outcomes in Patients With Type 2 Diabetes and Obesity
Abstract
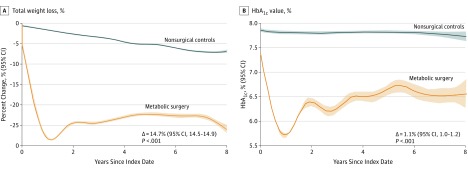
Importance: Although metabolic surgery (defined as procedures that influence metabolism by inducing weight loss and altering gastrointestinal physiology) significantly improves cardiometabolic risk factors, the effect on cardiovascular outcomes has been less well characterized.
Objective: To investigate the relationship between metabolic surgery and incident major adverse cardiovascular events (MACE) in patients with type 2 diabetes and obesity.
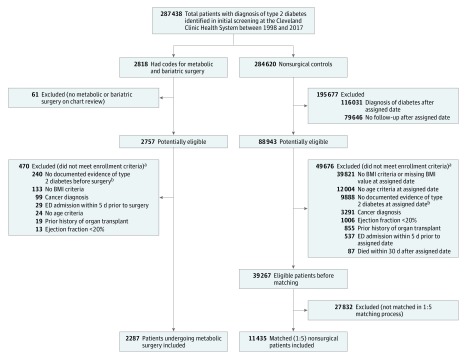
Design, setting, and participants: Of 287 438 adult patients with diabetes in the Cleveland Clinic Health System in the United States between 1998 and 2017, 2287 patients underwent metabolic surgery. In this retrospective cohort study, these patients were matched 1:5 to nonsurgical patients with diabetes and obesity (body mass index [BMI] ≥30), resulting in 11 435 control patients, with follow-up through December 2018.
Exposures: Metabolic gastrointestinal surgical procedures vs usual care for type 2 diabetes and obesity.
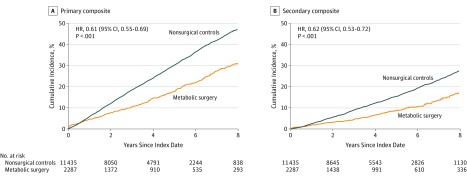
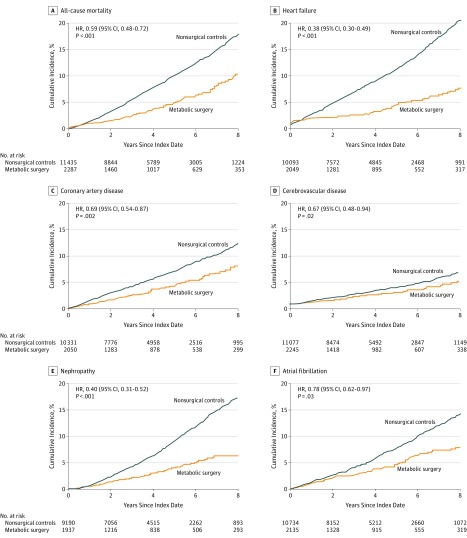
Main outcomes and measures: The primary outcome was the incidence of extended MACE (composite of 6 outcomes), defined as first occurrence of all-cause mortality, coronary artery events, cerebrovascular events, heart failure, nephropathy, and atrial fibrillation. Secondary end points included 3-component MACE (myocardial infarction, ischemic stroke, and mortality) and the 6 individual components of the primary end point.
Results: Among the 13 722 study participants, the distribution of baseline covariates was balanced between the surgical group and the nonsurgical group, including female sex (65.5% vs 64.2%), median age (52.5 vs 54.8 years), BMI (45.1 vs 42.6), and glycated hemoglobin level (7.1% vs 7.1%). The overall median follow-up duration was 3.9 years (interquartile range, 1.9-6.1 years). At the end of the study period, 385 patients in the surgical group and 3243 patients in the nonsurgical group experienced a primary end point (cumulative incidence at 8-years, 30.8% [95% CI, 27.6%-34.0%] in the surgical group and 47.7% [95% CI, 46.1%-49.2%] in the nonsurgical group [P < .001]; absolute 8-year risk difference [ARD], 16.9% [95% CI, 13.1%-20.4%]; adjusted hazard ratio [HR], 0.61 [95% CI, 0.55-0.69]). All 7 prespecified secondary outcomes showed statistically significant differences in favor of metabolic surgery, including mortality. All-cause mortality occurred in 112 patients in the metabolic surgery group and 1111 patients in the nonsurgical group (cumulative incidence at 8 years, 10.0% [95% CI, 7.8%-12.2%] and 17.8% [95% CI, 16.6%-19.0%]; ARD, 7.8% [95% CI, 5.1%-10.2%]; adjusted HR, 0.59 [95% CI, 0.48-0.72]).
Conclusions and relevance: Among patients with type 2 diabetes and obesity, metabolic surgery, compared with nonsurgical management, was associated with a significantly lower risk of incident MACE. The findings from this observational study must be confirmed in randomized clinical trials.
Trial registration: ClinicalTrials.gov Identifier: NCT03955952.
Conflict of interest statement
Figures
Comment in
- doi: 10.1001/jama.2019.14577
References
-
- Ikramuddin S, Korner J, Lee WJ, et al. . Lifestyle intervention and medical management with vs without Roux-en-Y gastric bypass and control of hemoglobin A1c, LDL cholesterol, and systolic blood pressure at 5 years in the Diabetes Surgery Study. JAMA. 2018;319(3):266-278. doi:10.1001/jama.2017.20813 - DOI - PMC - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, et al. . Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet. 2015;386(9997):964-973. doi:10.1016/S0140-6736(15)00075-6 - DOI - PubMed
-
- Johnson BL, Blackhurst DW, Latham BB, et al. . Bariatric surgery is associated with a reduction in major macrovascular and microvascular complications in moderately to severely obese patients with type 2 diabetes mellitus. J Am Coll Surg. 2013;216(4):545-556. doi:10.1016/j.jamcollsurg.2012.12.019 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
