

Intracranial actinomycosis of odontogenic origin masquerading as auto-immune orbital myositis: a fatal case and review of the literature
- PMID: 31477035
- PMCID: PMC6720412
- DOI: 10.1186/s12879-019-4408-2
Intracranial actinomycosis of odontogenic origin masquerading as auto-immune orbital myositis: a fatal case and review of the literature
Abstract
Background: Actinomycetes can rarely cause intracranial infection and may cause a variety of complications. We describe a fatal case of intracranial and intra-orbital actinomycosis of odontogenic origin with a unique presentation and route of dissemination. Also, we provide a review of the current literature.
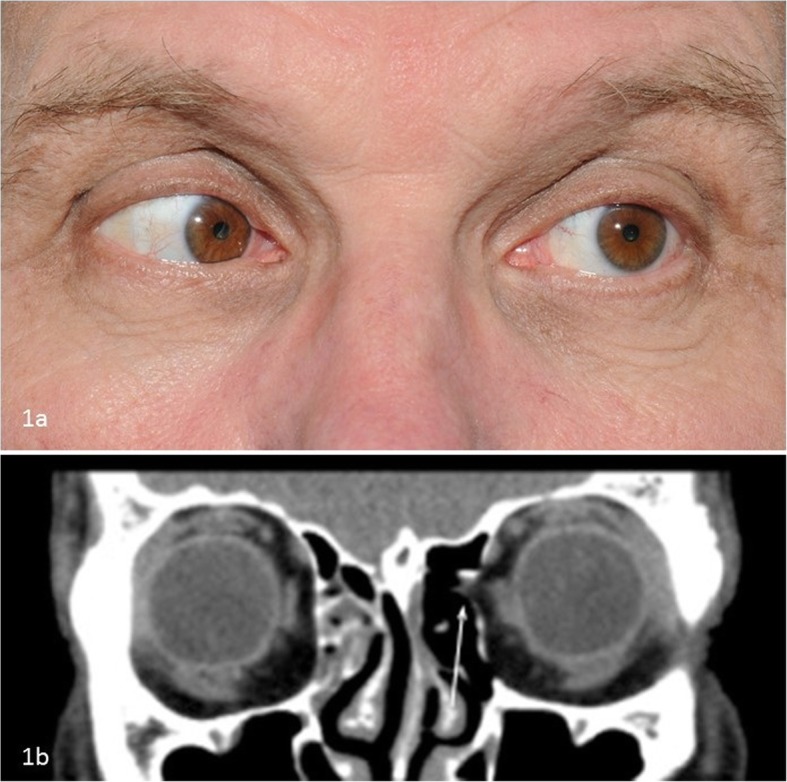
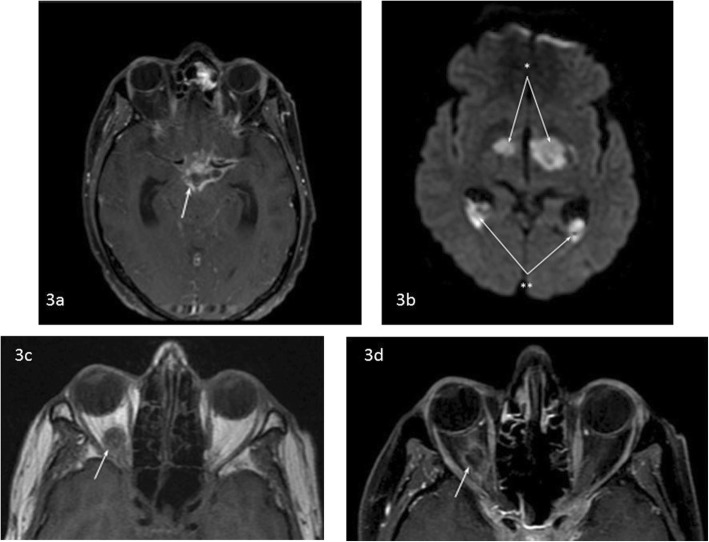
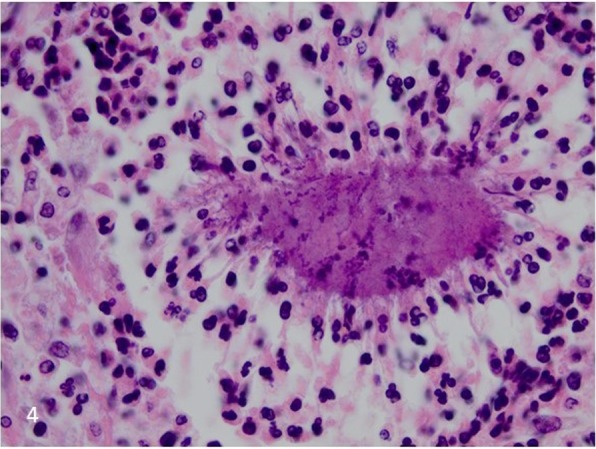
Case presentation: A 58-year-old man presented with diplopia and progressive pain behind his left eye. Six weeks earlier he had undergone a dental extraction, followed by clindamycin treatment for a presumed maxillary infection. The diplopia responded to steroids but recurred after cessation. The diplopia was thought to result from myositis of the left medial rectus muscle, possibly related to a defect in the lamina papyracea. During exploration there was no abnormal tissue for biopsy. The medial wall was reconstructed and the myositis responded again to steroids. Within weeks a myositis on the right side occurred, with CT evidence of muscle swelling. Several months later he presented with right hemiparesis and dysarthria. Despite treatment the patient deteriorated, developed extensive intracranial hemorrhage, and died. Autopsy showed bacterial aggregates suggestive of actinomycotic meningoencephalitis with septic thromboembolism. Retrospectively, imaging studies showed abnormalities in the left infratemporal fossa and skull base and bilateral cavernous sinus.
Conclusions: In conclusion, intracranial actinomycosis is difficult to diagnose, with potentially fatal outcome. An accurate diagnosis can often only be established by means of histology and biopsy should be performed whenever feasible. This is the first report of actinomycotic orbital involvement of odontogenic origin, presenting initially as bilateral orbital myositis rather than as orbital abscess. Infection from the upper left jaw extended to the left infratemporal fossa, skull base and meninges and subsequently to the cavernous sinus and the orbits.
Keywords: Actinomycosis; Intracranial infection; Intraorbital infection; Odontogenic origin; Orbital myositis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Myositis of the superior oblique muscle in a patient with suspected superior oblique muscle palsy.J AAPOS. 2023 Apr;27(2):102-105. doi: 10.1016/j.jaapos.2022.11.021. Epub 2023 Feb 10. J AAPOS. 2023. PMID: 36773743
-
Myositis of an Extraocular Muscle, a Possible Drug Reaction: Histopathologic and Immunopathologic Analysis.Ophthalmic Plast Reconstr Surg. 2021 Jul-Aug 01;37(4):e141-e143. doi: 10.1097/IOP.0000000000001923. Ophthalmic Plast Reconstr Surg. 2021. PMID: 33587420
-
An unusual manifestation of actinomycosis infection of the maxilla.Gen Dent. 2008 Mar-Apr;56(2):191-3. Gen Dent. 2008. PMID: 18348380
-
Recurrent bilateral orbital myositis: case report and review of the literature.Ann Trop Paediatr. 2011;31(2):173-80. doi: 10.1179/1465328111Y.0000000004. Ann Trop Paediatr. 2011. PMID: 21575325 Review.
-
Orbital myositis: diagnosis and management.Curr Allergy Asthma Rep. 2009 Jul;9(4):316-23. doi: 10.1007/s11882-009-0045-y. Curr Allergy Asthma Rep. 2009. PMID: 19656480 Review.
Cited by
-
Extensive actinomycosis with intracranial and mediastinal involvement: a therapeutic challenge.BMJ Case Rep. 2022 Aug 18;15(8):e247694. doi: 10.1136/bcr-2021-247694. BMJ Case Rep. 2022. PMID: 35981749 Free PMC article.
-
Postextraction infections, prevention, and treatment.Hua Xi Kou Qiang Yi Xue Za Zhi. 2024 Aug 1;42(4):426-434. doi: 10.7518/hxkq.2024.2023427. Hua Xi Kou Qiang Yi Xue Za Zhi. 2024. PMID: 39049629 Free PMC article. Chinese, English.
-
Heat Stress Affects Jejunal Immunity of Yellow-Feathered Broilers and Is Potentially Mediated by the Microbiome.Front Physiol. 2022 May 23;13:913696. doi: 10.3389/fphys.2022.913696. eCollection 2022. Front Physiol. 2022. PMID: 35677094 Free PMC article.
-
A case report on recurrent alternating Tolosa-Hunt syndrome due to bacterial sphenoid sinusitis: rediscussing the diagnostic terminology and classification.BMC Neurol. 2023 Jan 17;23(1):25. doi: 10.1186/s12883-023-03067-z. BMC Neurol. 2023. PMID: 36650509 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
