

Combination of CEUS and MRI for the diagnosis of periampullary space-occupying lesions: a retrospective analysis
- PMID: 31477041
- PMCID: PMC6719361
- DOI: 10.1186/s12880-019-0376-7
Combination of CEUS and MRI for the diagnosis of periampullary space-occupying lesions: a retrospective analysis
Abstract
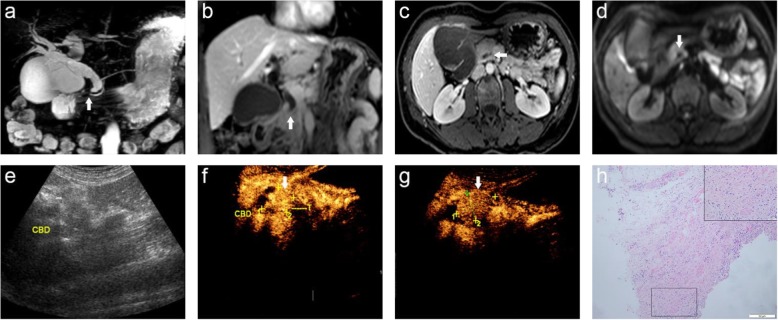
Background: The value of magnetic resonance imaging (MRI), contrast-enhanced ultrasound (CEUS), and the combination of CEUS and MRI (CCWM) for the diagnosis of periampullary space-occupying lesions (PSOL) was investigated.
Methods: A total of 102 patients diagnosed with PSOLs by surgery or biopsy were recruited retrospectively. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of MRI, CEUS, and CCWM were analyzed.
Results: MRI, CEUS, and CCWM allowed for the accurate detection of 91.17, 92.15, and 99.01% of PSOLs, respectively. The specificity, PPV, and accuracy of CCWM were significantly different from MRI and CEUS (p < 0.05). However, there the sensitivity and NPV were not significantly different among the three diagnostic technologies. In addition, the specificity, PPV, and accuracy were not significantly different between MRI and CEUS (all p > 0.05).
Conclusions: CCWM is valuable for differentiating benign and malignant PSOL, which provides important guiding significances for the clinic.
Keywords: CCMW; Contrast-enhanced ultrasound (CEUS); Magnetic resonance imaging (MRI); Periampullary cancer; Periampullary space-occupying lesions.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Baghmar S, Agrawal N, Kumar G, Bihari C, Patidar Y, Kumar S, et al. Prognostic factors and the role of adjuvant treatment in Periampullary carcinoma: a single-Centre experience of 95 patients. J Gastrointest Cancer. 2018. - PubMed
-
- Hashemzadeh Shahryar, Mehrafsa Behzad, Kakaei Farzad, Javadrashid Reza, Golshan Rosa, Seifar Fatemeh, Hajibonabi Farid, Salmannezhad Khorami Farzad. Diagnostic Accuracy of a 64-Slice Multi-Detector CT Scan in the Preoperative Evaluation of Periampullary Neoplasms. Journal of Clinical Medicine. 2018;7(5):91. doi: 10.3390/jcm7050091. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
