

Borderline pulmonary hypertension is associated with exercise intolerance and increased risk for acute exacerbation in patients with interstitial lung disease
- PMID: 31477076
- PMCID: PMC6721184
- DOI: 10.1186/s12890-019-0932-5
Borderline pulmonary hypertension is associated with exercise intolerance and increased risk for acute exacerbation in patients with interstitial lung disease
Abstract
Background: Pulmonary hypertension (PH) is traditionally defined as a resting mean pulmonary artery pressure (mPAP) of ≥25 mmHg, while mPAP in the range of 21 to 24 mmHg is recognized as "borderline PH." Interstitial lung disease (ILD) is complicated by the development of PH, which is known to be linked with exercise intolerance and a poor prognosis. Even though it has recently been recommended that PH is redefined as a mPAP of > 20 mmHg, little is known about the clinical significance of borderline PH in ILD. We evaluated whether borderline PH has an impact on the exercise capacity, risk of acute exacerbation (AE), and mortality in patients with ILD.
Methods: A total of 80 patients with ILD who underwent right heart catheterization (RHC) between November 2013 and October 2016 were included. The patients were divided into 3 groups according to the mPAP values: mPAP ≤20 mmHg (No-PH group; n = 56), 20 < mPAP < 25 mmHg (Bo-PH group; n = 18), and mPAP ≥25 mmHg (PH group; n = 6). The demographic, hemodynamic, spirometric, and 6-min walk test (6MWT) data of the patients were collected. In addition, the 1-year incidence of AEs and 1-year survival of the patients after the initial RHC were also evaluated.
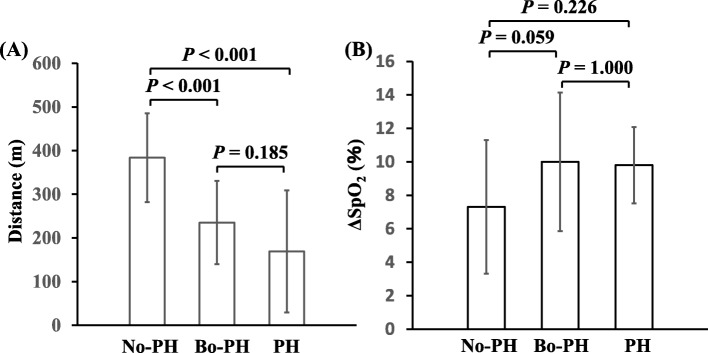
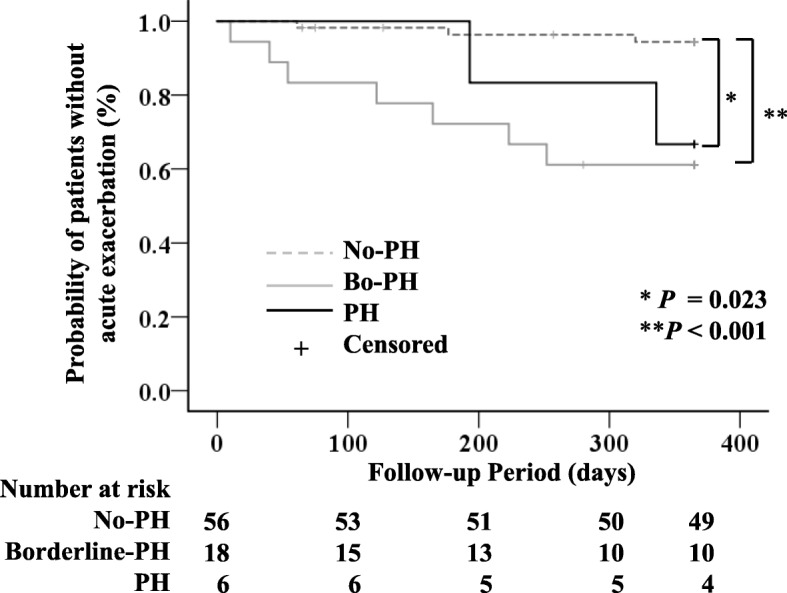
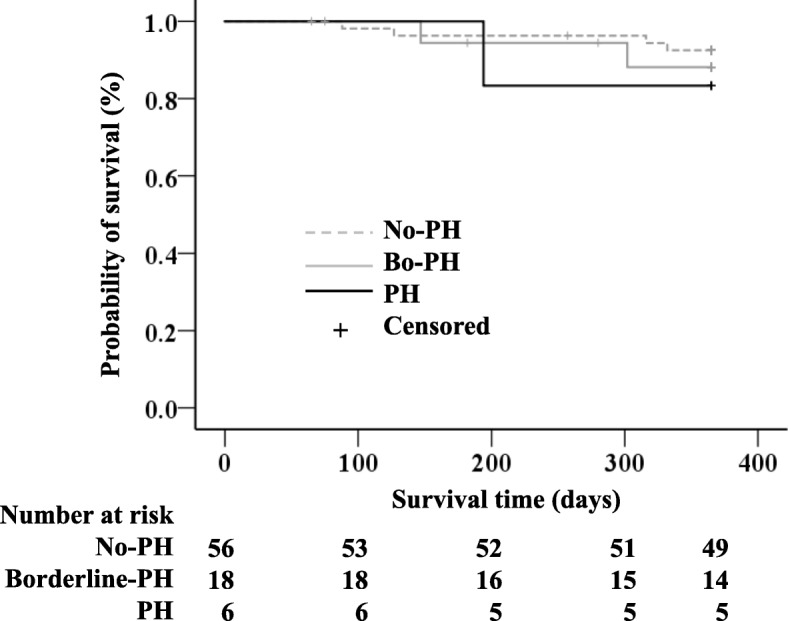
Results: There were no significant differences among the 3 groups in the mean age, pulmonary function parameters or the PaO2, however, 6-min walk distance was significantly lower in both the Bo-PH and PH groups (p < 0.001 for both) as compared to the No-PH group. The results of the Kaplan-Meier analysis revealed that while there was no significant difference in the 1-year survival rate among the three groups, the 1-year incidence of AEs was significantly higher in both the Bo-PH and PH groups (p < 0.001, p = 0.023, respectively) as compared to the No-PH group.
Conclusions: The current study suggested that borderline PH may be associated with poorer exercise tolerance and an increased risk of AEs in patients with ILD. Therefore, the physicians should pay close attention to the presence of even mild elevation of the mPAP at the initial evaluation in patients with ILD.
Keywords: 6-min walk test; Acute exacerbation; Borderline pulmonary hypertension; Interstitial lung disease; Pulmonary hypertension.
Conflict of interest statement
The all authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
