

Cardiopulmonary Exercise Testing Following Open Repair for a Proximal Thoracic Aortic Aneurysm or Dissection
- PMID: 31478921
- PMCID: PMC7048630
- DOI: 10.1097/HCR.0000000000000446
Cardiopulmonary Exercise Testing Following Open Repair for a Proximal Thoracic Aortic Aneurysm or Dissection
Abstract
Purpose: There are limited data on cardiopulmonary exercise testing (CPX) and cardiorespiratory fitness (CRF), following open repair for a proximal thoracic aortic aneurysm or dissection. The aim was to evaluate serious adverse events, abnormal CPX event rate, CRF (peak oxygen uptake, (Equation is included in full-text article.)O2peak), and blood pressure.
Methods: Patients were retrospectively identified from cardiac rehabilitation participation or prospectively enrolled in a research study and grouped by phenotype: (1) bicuspid aortic valve/thoracic aortic aneurysm, (2) tricuspid aortic valve/thoracic aortic aneurysm, and (3) acute type A aortic dissection.
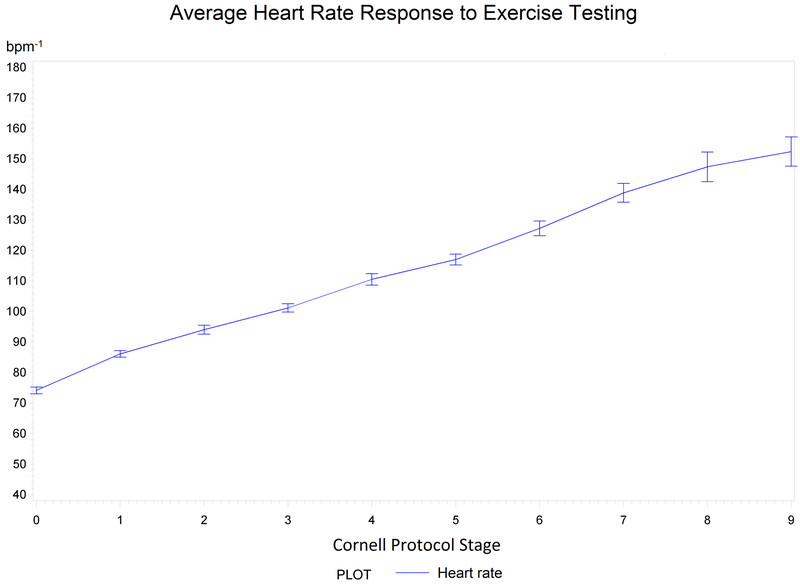
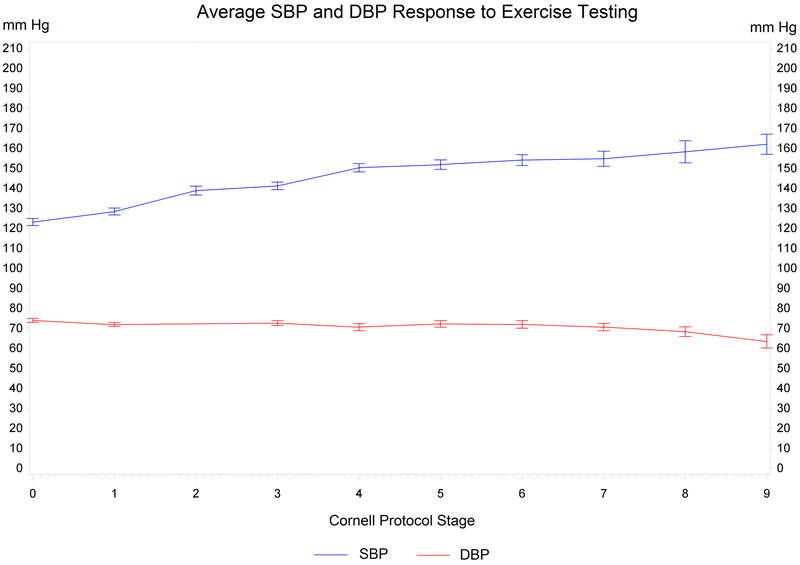
Results: Patients (n = 128) completed a CPX a median of 2.9 mo (interquartile range: 1.8, 3.5) following repair. No serious adverse events were reported, although 3 abnormal exercise tests (2% event rate) were observed. Eighty-one percent of CPX studies were considered peak effort (defined as respiratory exchange ratio of ≥1.05). Median measured (Equation is included in full-text article.)O2peak was <36% predicted normative values (19.2 mL·kgmin vs 29.3 mLkgmin, P < .0001); the most marked impairment in (Equation is included in full-text article.)O2peak was observed in the acute type A aortic dissection group (<40% normative values), which was significantly different from other groups (P < .05). Peak exercise systolic and diastolic blood pressures were 160 mm Hg (144, 172) and 70 mm Hg (62, 80), with no differences noted between groups.
Conclusions: We observed no serious adverse events with an abnormal CPX event rate of only 2% 3 mo following repair for a proximal thoracic aortic aneurysm or dissection. (Equation is included in full-text article.)O2peak was reduced among all patient groups, especially the acute type A aortic dissection group, which may be clinically significant, given the well-established prognostic importance of reduced cardiorespiratory fitness.
Conflict of interest statement
Conflicts of Interest
Himanshu J. Patel is a consultant for WL gore Edwards and Medtronic.
Figures
References
-
- Olsson C, Thelin S, Stahle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114(24):2611–2618. - PubMed
-
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(41):2873–2926. - PubMed
-
- ACSM’s Guidelines for Exercise Testing and Prescription 10th ed: Wolters Kluwer; 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
