

Temporal Trends and Patterns in Mortality After Incident Heart Failure: A Longitudinal Analysis of 86 000 Individuals
- PMID: 31479100
- PMCID: PMC6724155
- DOI: 10.1001/jamacardio.2019.3593
Temporal Trends and Patterns in Mortality After Incident Heart Failure: A Longitudinal Analysis of 86 000 Individuals
Abstract
Importance: Despite considerable improvements in heart failure care, mortality rates among patients in high-income countries have changed little since the early 2000s. Understanding the reasons underlying these trends may provide valuable clues for developing more targeted therapies and public health strategies.
Objective: To investigate mortality rates following a new diagnosis of heart failure and examine changes over time and by cause of death and important patient features.
Design, setting, and participants: This population-based retrospective cohort study analyzed anonymized electronic health records of individuals who received a new diagnosis of heart failure between January 2002 and December 2013 who were followed up until December 2014 from the Clinical Practice Research Datalink, which links information from primary care, secondary care, and the national death registry from a subset of the UK population. The data were analyzed from January 2018 to February 2019.
Main outcomes and measures: All-cause and cause-specific mortality rates at 1 year following diagnosis. Poisson regression models were used to calculate rate ratios (RRs) and 95% confidence intervals comparing 2013 with 2002, adjusting for age, sex, region, socioeconomic status, and 17 major comorbidities.
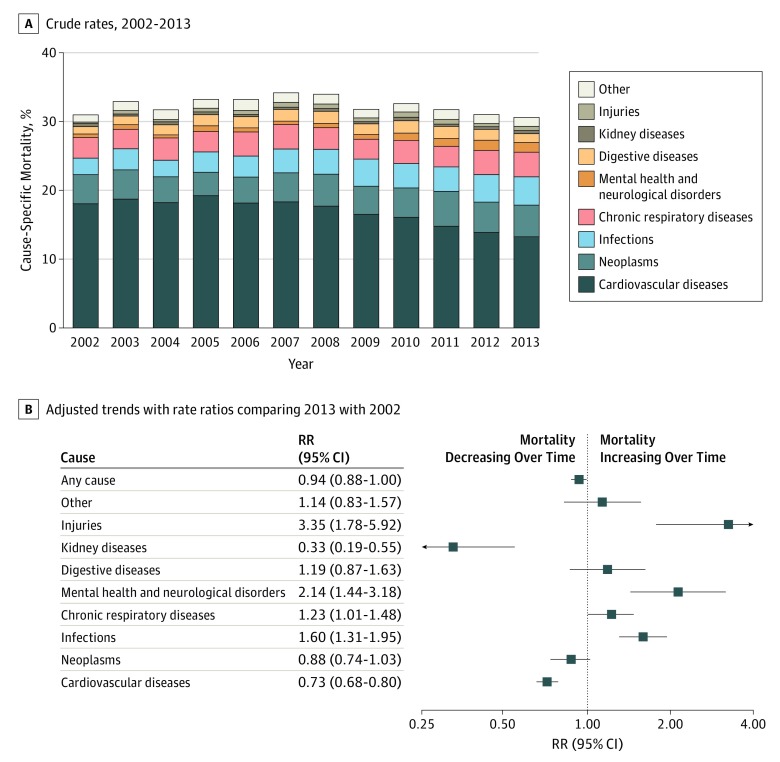
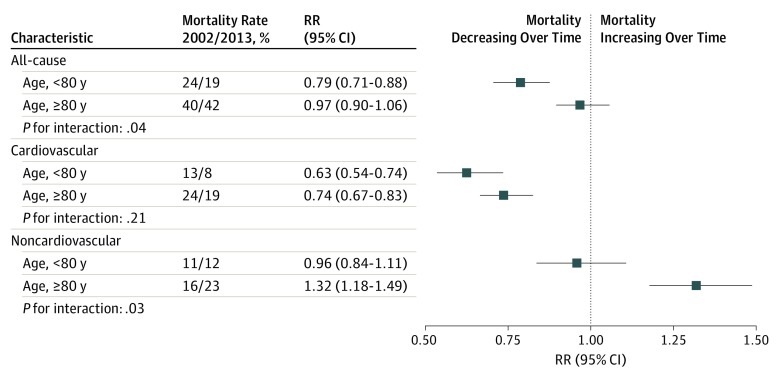
Results: Of 86 833 participants, 42 581 (49%) were women, 51 215 (88%) were white, and the mean (SD) age was 76.6 (12.6) years. While all-cause mortality rates declined only modestly over time (RR comparing 2013 with 2002, 0.94; 95% CI, 0.88-1.00), underlying patterns presented explicit trends. A decline in cardiovascular mortality (RR, 0.73; 95% CI, 0.67-0.80) was offset by an increase in noncardiovascular deaths (RR, 1.22; 95% CI, 1.11-1.33). Subgroup analyses further showed that overall mortality rates declined among patients younger than 80 years (RR, 0.79; 95% CI, 0.71-0.88) but not among those older than 80 years (RR, 0.97; 95% CI, 0.90-1.06). After cardiovascular causes (898 [43%]), the major causes of death in 2013 were neoplasms (311 [15%]), respiratory conditions (243 [12%]), and infections (13%), the latter 2 explaining most of the observed increase in noncardiovascular mortality.
Conclusions and relevance: Among patients with a new heart failure diagnosis, considerable progress has been achieved in reducing mortality in young and middle-aged patients and cardiovascular mortality across all age groups. Improvements to overall mortality are hindered by high and increasing rates of noncardiovascular events. These findings challenge current research priorities and management strategies and call for a greater emphasis on associated comorbidities. Specifically, infection prevention presents as a major opportunity to improve prognosis.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
