

Safety and Efficacy of Dabigatran Etexilate vs Dose-Adjusted Warfarin in Patients With Cerebral Venous Thrombosis: A Randomized Clinical Trial
- PMID: 31479105
- PMCID: PMC6724157
- DOI: 10.1001/jamaneurol.2019.2764
Safety and Efficacy of Dabigatran Etexilate vs Dose-Adjusted Warfarin in Patients With Cerebral Venous Thrombosis: A Randomized Clinical Trial
Abstract
Importance: Patients with cerebral venous thrombosis (CVT) are at risk of recurrent venous thrombotic events (VTEs). Non-vitamin K oral anticoagulants have not been evaluated in randomized controlled trials in CVT.
Objective: To compare the efficacy and safety of dabigatran etexilate with those of dose-adjusted warfarin in preventing recurrent VTEs in patients who have experienced a CVT.
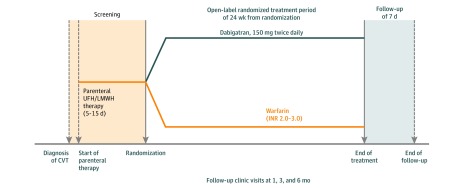
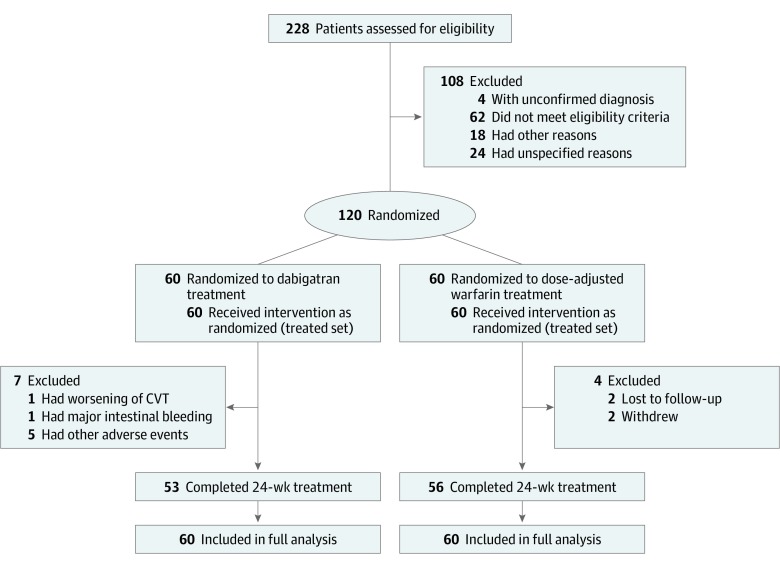
Design, setting, and participants: RE-SPECT CVT is an exploratory, prospective, randomized (1:1), parallel-group, open-label, multicenter clinical trial with blinded end-point adjudication (PROBE design). It was performed from December 21, 2016, to June 22, 2018, with a follow-up of 25 weeks, at 51 tertiary sites in 9 countries (France, Germany, India, Italy, the Netherlands, Poland, Portugal, Russia, and Spain). Adult consecutive patients with acute CVT, who were stable after 5 to 15 days of treatment with parenteral heparin, were screened for eligibility. Patients with CVT associated with central nervous system infection or major trauma were excluded, but those with intracranial hemorrhage from index CVT were allowed to participate. After exclusions, 120 patients were randomized. Data were analyzed following the intention-to-treat approach.
Interventions: Dabigatran, 150 mg twice daily, or dose-adjusted warfarin for a treatment period of 24 weeks.
Main outcomes and measures: Primary outcome was a composite of patients with a new VTE (recurrent CVT, deep vein thrombosis of any limb, pulmonary embolism, and splanchnic vein thrombosis) or major bleeding during the study period. Secondary outcomes were cerebral venous recanalization and clinically relevant non-major bleeding events.
Results: In total, 120 patients with CVT were randomized to the 2 treatment groups (60 to dabigatran and 60 to dose-adjusted warfarin). Of the randomized patients, the mean (SD) age was 45.2 (13.8) years, and 66 (55.0%) were women. The mean (SD) duration of exposure was 22.3 (6.16) weeks for the dabigatran group and 23.0 (5.20) weeks for the warfarin group. No recurrent VTEs were observed. One (1.7%; 95% CI, 0.0-8.9) major bleeding event (intestinal) was recorded in the dabigatran group, and 2 (3.3%; 95% CI, 0.4-11.5) (intracranial) in the warfarin group. One additional patient (1.7; 95% CI, 0.0-8.9) in the warfarin group experienced a clinically relevant non-major bleeding event. Recanalization occurred in 33 patients in the dabigatran group (60.0%; 95% CI, 45.9-73.0) and in 35 patients in the warfarin group (67.3%; 95% CI, 52.9-79.7).
Conclusions and relevance: This trial found that patients who had CVT anticoagulated with either dabigatran or warfarin had low risk of recurrent VTEs, and the risk of bleeding was similar with both medications, suggesting that both dabigatran and warfarin may be safe and effective for preventing recurrent VTEs in patients with CVT.
Trial registration: ClinicalTrials.gov identifier: NCT02913326.
Conflict of interest statement
Figures
References
-
- Janghorbani M, Zare M, Saadatnia M, Mousavi SA, Mojarrad M, Asgari E. Cerebral vein and dural sinus thrombosis in adults in Isfahan, Iran: frequency and seasonal variation. Acta Neurol Scand. 2008;117(2):117-121. - PubMed
-
- Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators . Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004;35(3):664-670. doi:10.1161/01.STR.0000117571.76197.26 - DOI - PubMed
