

Effect of Low-Intensity vs Standard-Intensity Warfarin Prophylaxis on Venous Thromboembolism or Death Among Patients Undergoing Hip or Knee Arthroplasty: A Randomized Clinical Trial
- PMID: 31479138
- PMCID: PMC6724181
- DOI: 10.1001/jama.2019.12085
Effect of Low-Intensity vs Standard-Intensity Warfarin Prophylaxis on Venous Thromboembolism or Death Among Patients Undergoing Hip or Knee Arthroplasty: A Randomized Clinical Trial
Abstract
Importance: The optimal international normalized ratio (INR) to prevent venous thromboembolism (VTE) in warfarin-treated patients with recent arthroplasty is unknown.
Objective: To determine the safety and efficacy of a target INR of 1.8 vs 2.5 for VTE prophylaxis after orthopedic surgery.
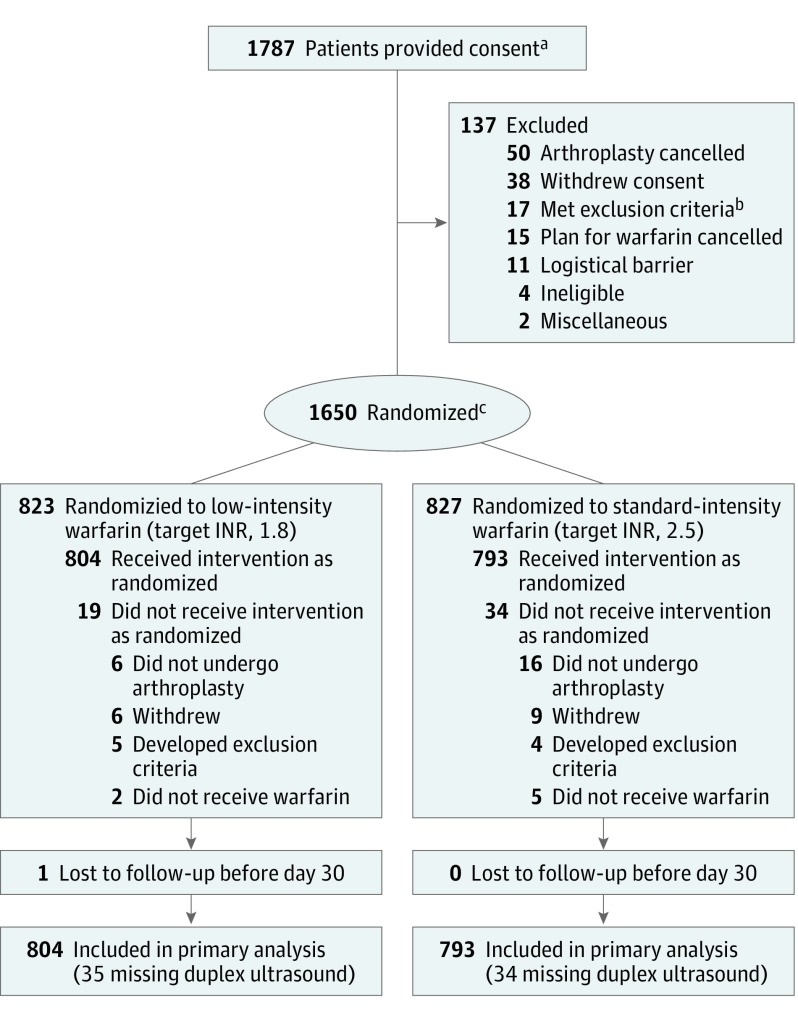
Design, setting, and participants: The randomized Genetic Informatics Trial (GIFT) of Warfarin to Prevent Deep Vein Thrombosis enrolled 1650 patients aged 65 years or older initiating warfarin for elective hip or knee arthroplasty at 6 US medical centers. Enrollment began in April 2011 and follow-up concluded in October 2016.
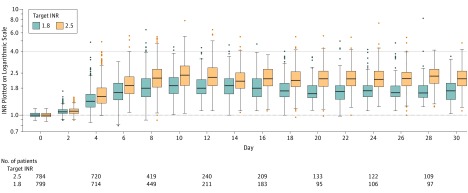
Interventions: In a 2 × 2 factorial design, participants were randomized to a target INR of 1.8 (n = 823) or 2.5 (n = 827) and to either genotype-guided or clinically guided warfarin dosing. For the first 11 days of therapy, open-label warfarin dosing was guided by a web application.
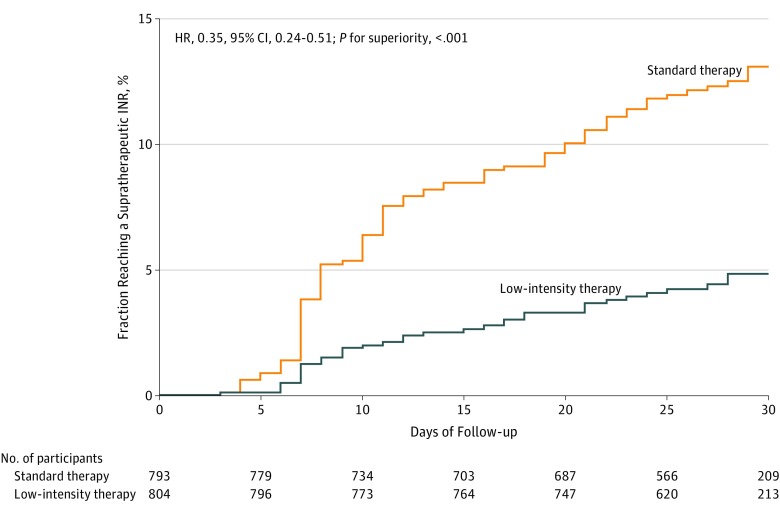
Main outcomes and measures: The primary outcome was the composite of VTE (within 60 days) or death (within 30 days). Participants underwent screening duplex ultrasound postoperatively. The hypothesis was that an INR target of 1.8 would be noninferior to an INR target of 2.5, using a noninferiority margin of 3% for the absolute risk of VTE. Secondary end points were bleeding and INR values of 4 or more.
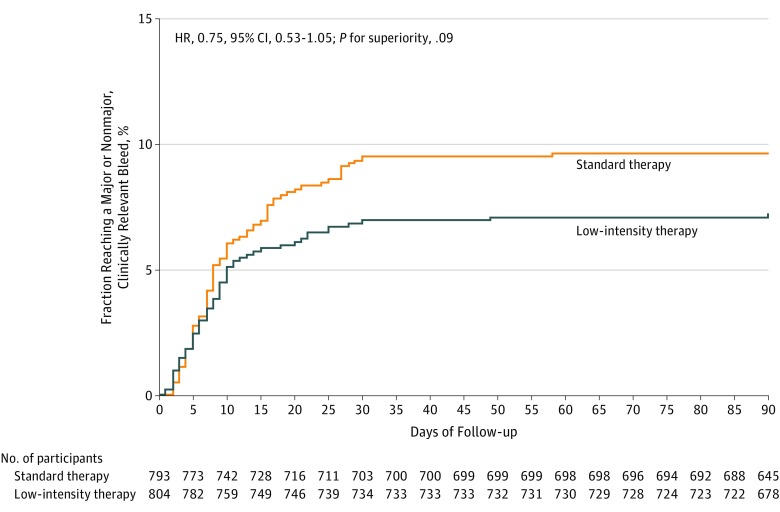
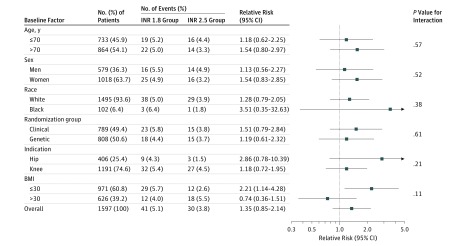
Results: Among 1650 patients who were randomized (mean age, 72.1 years; 1049 women [63.6%]; 1502 white [91.0%]), 1597 (96.8%) received at least 1 dose of warfarin and were included in the primary analysis. The rate of the primary composite outcome of VTE or death was 5.1% (41 of 804) in the low-intensity-warfarin group (INR target, 1.8) vs 3.8% (30 of 793) in the standard-treatment-warfarin group (INR target, 2.5), for a difference of 1.3% (1-sided 95% CI, -∞ to 3.05%, P = .06 for noninferiority). Major bleeding occurred in 0.4% of patients in the low-intensity group and 0.9% of patients in the standard-intensity group, for a difference of -0.5% (95% CI, -1.6% to 0.4%). The INR values of 4 or more occurred in 4.5% of patients in the low-intensity group and 12.2% of the standard-intensity group, for a difference of -7.8% (95% CI, -10.5% to -5.1%).
Conclusions and relevance: Among older patients undergoing hip or knee arthroplasty and receiving warfarin prophylaxis, an international normalized ratio goal of 1.8 compared with 2.5 did not meet the criterion for noninferiority for risk of the composite outcome of VTE or death. However, the trial may have been underpowered to meet this criterion and further research may be warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT01006733.
Conflict of interest statement
Figures
References
-
- Cieri NE, Kusmierski K, Lackie C, Van Opdorp A, Hassan AK. Retrospective evaluation of postoperative adverse drug events in patients receiving rivaroxaban after major orthopedic surgery compared with standard therapy in a community hospital. Pharmacotherapy. 2017;37(2):170-176. doi: 10.1002/phar.1888 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
