

Integrating preexposure prophylaxis delivery in routine family planning clinics: A feasibility programmatic evaluation in Kenya
- PMID: 31479452
- PMCID: PMC6719826
- DOI: 10.1371/journal.pmed.1002885
Integrating preexposure prophylaxis delivery in routine family planning clinics: A feasibility programmatic evaluation in Kenya
Abstract
Background: Young women account for a disproportionate fraction of new HIV infections in Africa and are a priority population for HIV prevention, including implementation of preexposure prophylaxis (PrEP). The overarching goal of this project was to demonstrate the feasibility of integrating PrEP delivery within routine family planning (FP) clinics to serve as a platform to efficiently reach at-risk adolescent girls and young women (AGYW) for PrEP in HIV high-burden settings.
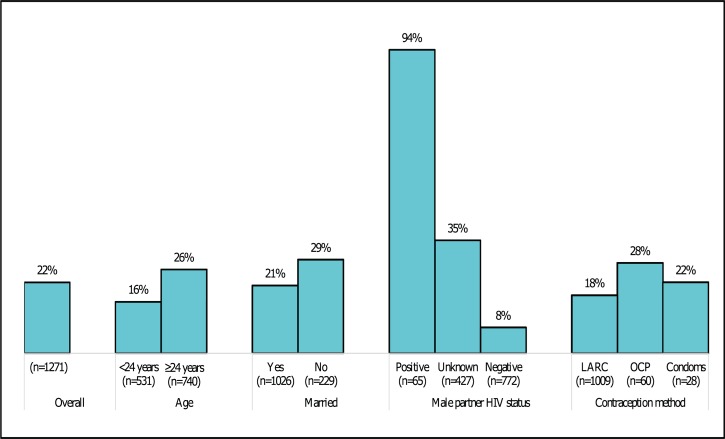
Methods and findings: The PrEP Implementation in Young Women and Adolescents (PrIYA) program is a real-world implementation program to demonstrate integration of PrEP delivery for at-risk AGYW in FP clinics in Kisumu, Kenya. Between November 2017 and June 2018, women aged 15 to 45 from the general population seeking FP services at 8 public health clinics were universally screened for HIV behavioral risk factors and offered PrEP following national PrEP guidelines. We evaluated PrEP uptake and continuation, and robust Poisson regression methods were used to identify correlates of uptake and early continuation of PrEP, with age included as a one-knot linear spline. Overall, 1,271 HIV-uninfected women accessing routine FP clinics were screened for PrEP; the median age was 25 years (interquartile range [IQR]: 22-29), 627 (49%) were <24 years old, 1,026 (82%) were married, more than one-third (34%) had partners of unknown HIV status, and the vast majority (n = 1,200 [94%]) reported recent condom-less sex. Of 1,271 women screened, 278 (22%) initiated PrEP, and 114 (41%) returned for at least one refill visit after initiation. PrEP uptake was independently associated with reported male-partner HIV status (HIV-positive 94%, unknown 35%, HIV-negative 8%; p < 0.001) and marital status (28% unmarried versus married 21%; p = 0.04), and a higher proportion of women ≥24 years (26%; 191/740) initiated PrEP compared to 16% (87/531) of young women <24 years (p < 0.001). There was a moderate and statistically non-significant unadjusted increase in PrEP uptake among women using oral contraception pills (OCPs) compared to women using injectable or long-acting reversible contraception methods (OCP 28% versus injectable/implants/intrauterine devices [IUDs] 18%; p = 0.06). Among women with at least one post-PrEP initiation follow-up visit (n = 278), no HIV infection was documented during the project period. Overall, continuation of PrEP use at 1, 3, and 6 months post initiation was 41%, 24%, and 15%, respectively. The likelihood for early continuation of PrEP use (i.e., return for at least one PrEP refill within 45 days post initiation) was strongly associated with reported male-partner HIV status (HIV-positive 67%, -negative 39%, unknown 31%; overall effect p = 0.001), and a higher proportion of women ≥24 years old continued PrEP at 1 month compared with young women <24 years old (47% versus 29%; p = 0.002). For women ≥24 years old, the likelihood to continue PrEP use at 1 month post initiation increased by 3% for each additional year of a woman's age (adjusted prevalence ratio [PR]: 1.03; 95% confidence interval [CI]: 1.01-1.05; p = 0.01). In contrast, for women <24 years old, the likelihood of continuing PrEP for each additional year of a woman's age was high in magnitude (approximately 6%) but statistically non-significant (adjusted PR: 1.06; 95% CI: 0.97-1.16; p = 0.18). Frequently reported reasons for discontinuing PrEP were low perceived risk of HIV (25%), knowledge that partner was HIV negative (24%), experiencing side effects (20%), and pill burden (17%). Study limitations include lack of qualitative work to provide insights into women's decision-making on PrEP uptake and continuation, the small number of measured covariates imposed by the program data, and a nonrandomized design limiting definitive ascertainment of the robustness of a PrEP-dedicated nurse-led implementation strategy.
Conclusions: In this real-world PrEP implementation program in Kenya, integration of universal screening and counseling for PrEP in FP clinics was feasible, making this platform a potential "one-stop" location for FP and PrEP. There was a high drop-off in PrEP continuation, but a subset of women continued PrEP use at least through 1 month, possibly indicating further reflection or decision-making on PrEP use. Greater efforts to support PrEP normalization and persistence for African women are needed to help women navigate their decisions about HIV prevention preferences as their reproductive goals and HIV vulnerability evolve.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: GJS received grants from NIH, CDC, Thrasher Foundation, and funding from UW, UpToDate, and IMPAACT; JMB is on advisory boards for Gilead Sciences, Merck, and Janssen. The authors have declared that no other competing interests exist.
Figures

References
-
- UNAIDS. The Gap Report Geneva, Switzerland: UNAIDS; 2016. Available from: http://www.unaids.org/sites/default/files/media_asset/2016-prevention-ga.... [cited 2019 Jul 28].
-
- Baeten JM, Donnell D, Mugo NR, Ndase P, Thomas KK, Campbell JD, et al. Single-agent tenofovir versus combination emtricitabine plus tenofovir for pre-exposure prophylaxis for HIV-1 acquisition: an update of data from a randomised, double-blind, phase 3 trial. Lancet Infect Dis. 2014;14(11):1055–64. Epub 2014/10/11 06:00. 10.1016/S1473-3099(14)70937-5 - DOI - PMC - PubMed
-
- Baeten JM, Heffron R, Kidoguchi L, Mugo NR, Katabira E, Bukusi EA, et al. Integrated delivery of antiretroviral treatment and pre-exposure prophylaxis to HIV-1-serodiscordant couples: a prospective implementation study in Kenya and Uganda. PLoS Med. 2016;13(8):e1002099 Epub 2016/08/24 06:00. 10.1371/journal.pmed.1002099 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
