

Relationship between protein biomarkers of chemotherapy response and microsatellite status, tumor mutational burden and PD-L1 expression in cancer patients
- PMID: 31479512
- PMCID: PMC7051881
- DOI: 10.1002/ijc.32661
Relationship between protein biomarkers of chemotherapy response and microsatellite status, tumor mutational burden and PD-L1 expression in cancer patients
Abstract
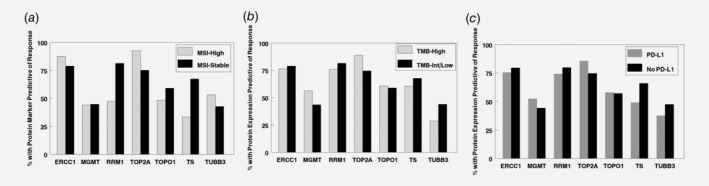
Chemotherapy and checkpoint inhibitor immunotherapies are increasingly used in combinations. We determined associations between the presence of anti-PD-1/PD-L1 therapeutic biomarkers and protein markers of potential chemotherapy response. Data were extracted from a clinical-grade testing database (Caris Life Sciences; February 2015 through November 2017): immunotherapy response markers (microsatellite instability-high [MSI-H], tumor mutational burden-high [TMB-H], and PD-L1 protein expression) and protein chemotherapy response markers (excision repair complementation group 1 [ERCC1], topoisomerase 1 [TOPO1], topoisomerase 2 [TOP2A], thymidylate synthase [TS], tubulin beta 3 [TUBB3], ribonucleotide reductase regulatory subunit M1 [RRM1] and O-6-methyl guanine DNA methyltransferase [MGMT]). Relationships were determined by the Mantel-Haenszel chi-squared test or Fischer's exact tests. Overall, 28,034 patients representing a total of 40 tumor types were assessed. MSI-H was found in 3.3% of patients (73% were also TMB-H), TMB-H, 8.4% (28.3% were also MSI-H) and PD-L1 expression in 11.0% of patients (5.1% were also MSI-H; 16.4% were also TMB-H). Based on concurrent biomarker expression, combinations of immunotherapy with platinum (ERCC1 negativity) or with doxorubicin, epirubicin or etoposide (TOP2A positivity) have a higher probability of response, whereas combinations with irinotecan or topotecan (TOPO1 positivity), with gemcitabine (RRM1 negativity), and fluorouracil, pemetrexed or capecitabine (TS negativity) may be of less benefit. The potential for immunotherapy and taxane (TUBB3 negativity) combinations is present for MSI-H but not TMB-H or PD-L1-expressing tumors; for temozolomide and dacarbazine (MGMT negative), PD-L1 is frequently coexpressed, but MSI-H and TMB-H are not associated. Protein markers of potential chemotherapy response along with next-generation sequencing for immunotherapy response markers can help support rational combinations as part of an individualized, precision oncology approach.
Keywords: MSI; PD-L1; TMB; cytotoxic chemotherapy; immunotherapy.
© 2019 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
