

Atopic Eczema in Adulthood and Risk of Depression and Anxiety: A Population-Based Cohort Study
- PMID: 31479767
- PMCID: PMC6947493
- DOI: 10.1016/j.jaip.2019.08.030
Atopic Eczema in Adulthood and Risk of Depression and Anxiety: A Population-Based Cohort Study
Abstract
Background: Atopic eczema is a common and debilitating condition associated with depression and anxiety, but the nature of this association remains unclear.
Objective: To explore the temporal relationship between atopic eczema and new depression/anxiety.
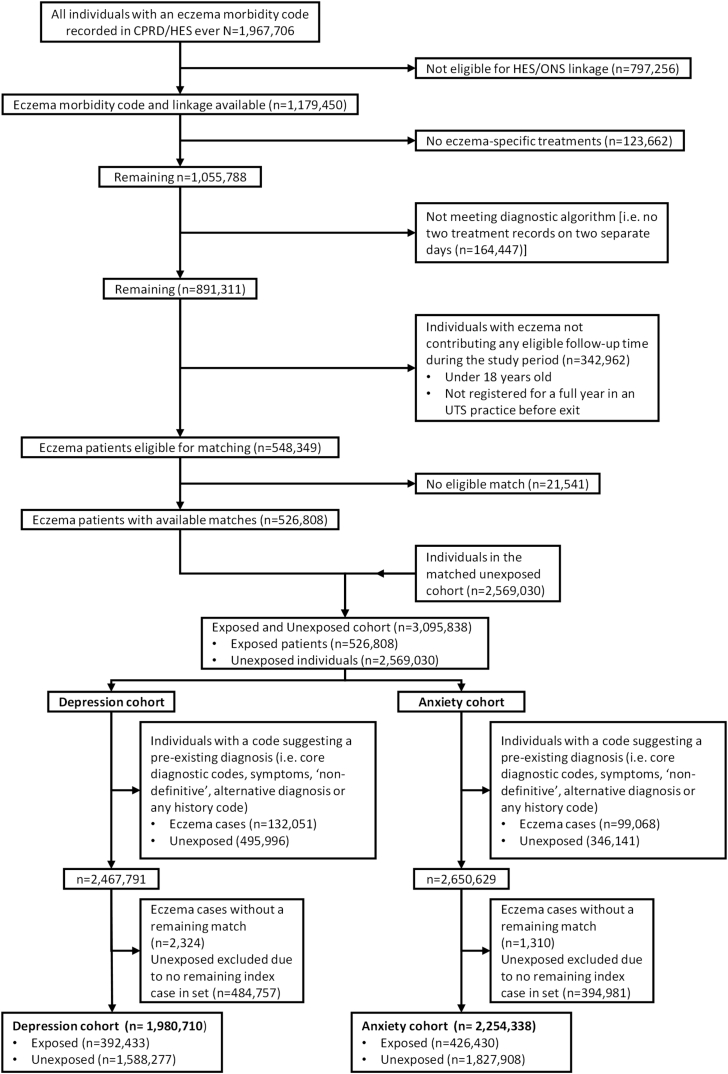
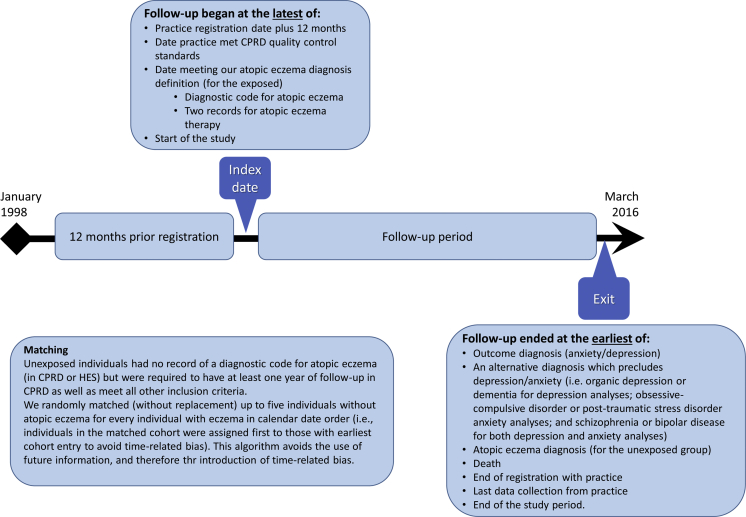
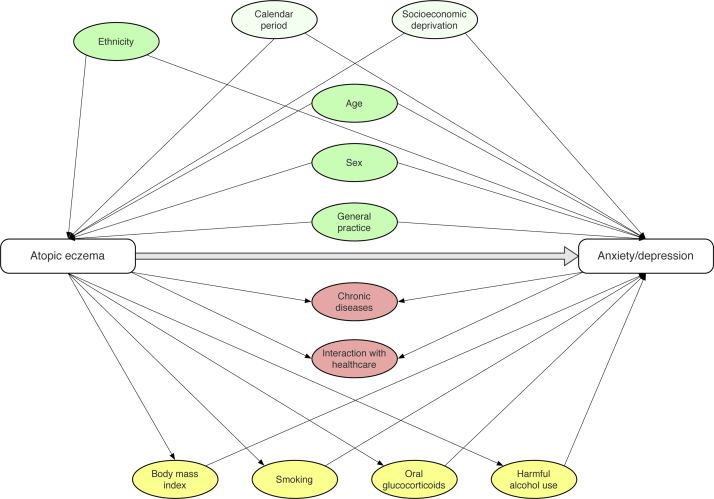
Methods: This matched cohort study used routinely collected data from the UK Clinical Practice Research Datalink, linked to hospital admissions data. We identified adults with atopic eczema (1998-2016) using a validated algorithm, and up to 5 individuals without atopic eczema matched on date of diagnosis, age, sex, and general practice. We estimated the hazard ratio (HR) for new depression/anxiety using stratified Cox regression to account for age, sex, calendar period, Index of Multiple Deprivation, glucocorticoid treatment, obesity, smoking, and harmful alcohol use.
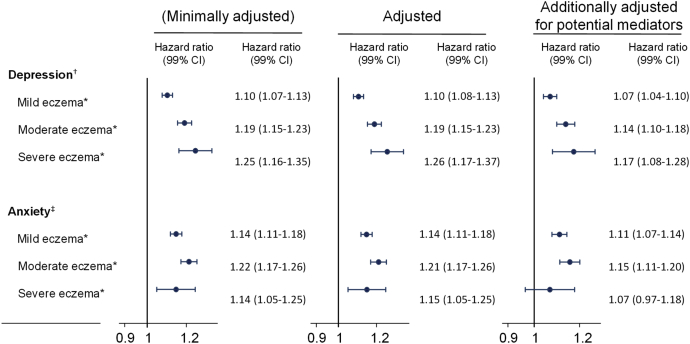
Results: We identified 526,808 adults with atopic eczema who were matched to 2,569,030 without. Atopic eczema was associated with increased incidence of new depression (HR, 1.14; 99% CI, 1.12-1.16) and anxiety (HR, 1.17; 99% CI, 1.14-1.19). We observed a stronger effect of atopic eczema on depression with increasing atopic eczema severity (HR [99% CI] compared with no atopic eczema: mild, 1.10 [1.08-1.13]; moderate, 1.19 [1.15-1.23]; and severe, 1.26 [1.17-1.37]). A dose-response association, however, was less apparent for new anxiety diagnosis (HR [99% CI] compared with no atopic eczema: mild, 1.14 [1.11-1.18]; moderate, 1.21 [1.17-1.26]; and severe, 1.15; [1.05-1.25]).
Conclusions: Adults with atopic eczema are more likely to develop new depression and anxiety. For depression, we observed a dose-response relationship with atopic eczema severity.
Keywords: Anxiety; Atopic dermatitis; Atopic eczema; Depression; Population-based; Severity.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Drucker A.M., Wang A.R., Li W.Q., Sevetson E., Block J.K., Qureshi A.A. The burden of atopic dermatitis: summary of a report for the National Eczema Association. J Invest Dermatol. 2017;137:26–30. - PubMed
-
- Weidinger S., Novak N. Atopic dermatitis. Lancet. 2016;387:1109–1122. - PubMed
-
- Odhiambo J.A., Williams H.C., Clayton T.O., Robertson C.F., Asher M.I. Global variations in prevalence of eczema symptoms in children from ISAAC phase three. J Allergy Clin Immunol. 2009;124:1251–1258.e23. - PubMed
-
- Silverberg J.I., Hanifin J.M. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. J Allergy Clin Immunol. 2013;132:1132–1138. - PubMed
-
- Wollenberg A., Barbarot S., Bieber T., Christen-Zaech S., Deleuran M., Fink-Wagner A. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. J Eur Acad Dermatology Venereol. 2018;32:850–878. - PubMed
