

Bone Diseases in Patients with Chronic Liver Disease
- PMID: 31480433
- PMCID: PMC6747370
- DOI: 10.3390/ijms20174270
Bone Diseases in Patients with Chronic Liver Disease
Abstract
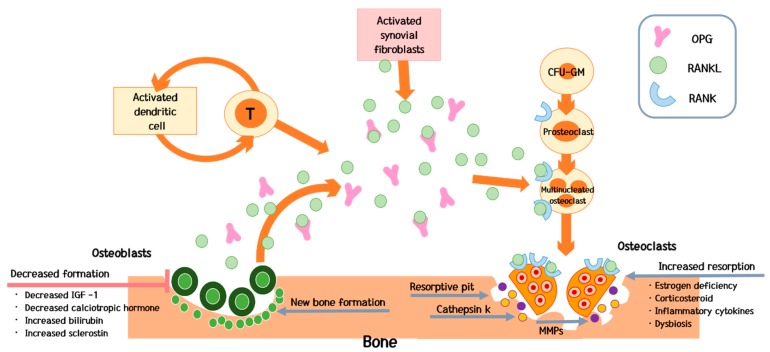
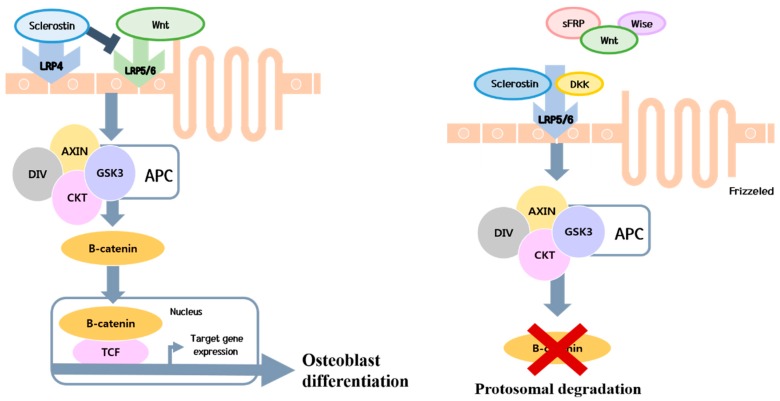
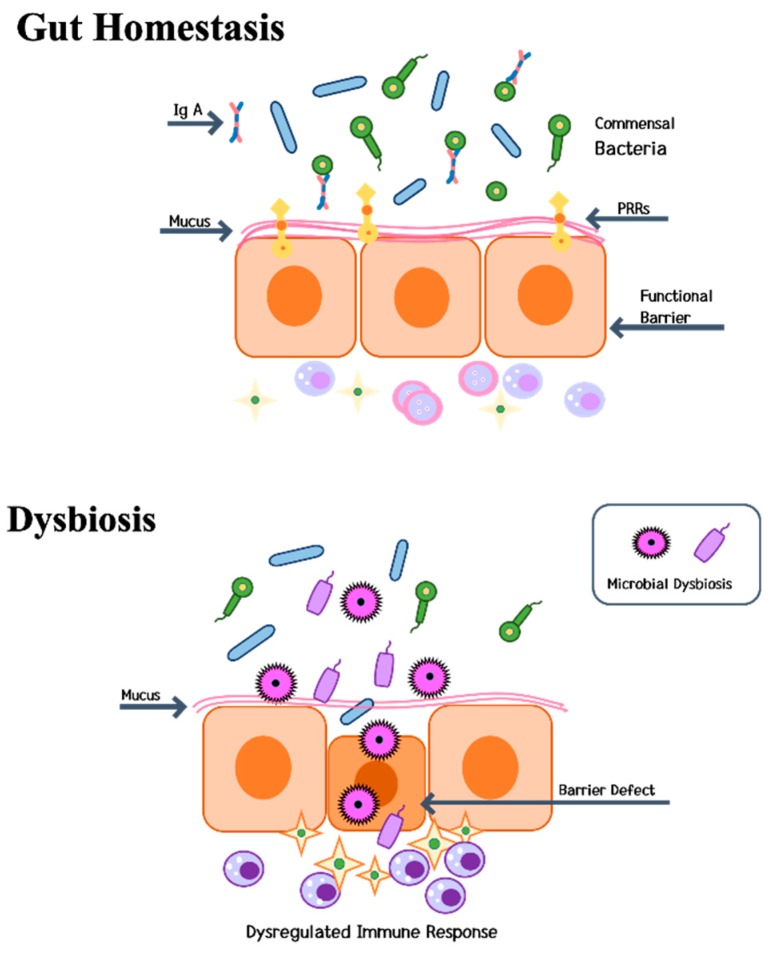
Osteoporosis is a frequently observed complication in patients with chronic liver disease, particularly liver cirrhosis and cholestatic liver diseases. In addition, osteoporosis is critical in patients receiving a liver transplant. Nevertheless, few studies have evaluated bone diseases in patients with more frequently observed chronic liver disease, such as chronic viral hepatitis, nonalcoholic fatty liver disease and alcoholic liver disease. Osteoporosis is a disease caused by an imbalance in the activities of osteoblasts and osteoclasts. Over the last few decades, many advances have improved our knowledge of the pathogenesis of osteoporosis. Importantly, activated immune cells affect the progression of osteoporosis, and chronic inflammation may exert an additional effect on the existing pathophysiology of osteoporosis. The microbiota of the intestinal tract may also affect the progression of bone loss in patients with chronic liver disease. Recently, studies regarding the effects of chronic inflammation on dysbiosis in bone diseases have been conducted. However, mechanisms underlying osteoporosis in patients with chronic liver disease are complex and precise mechanisms remain unknown. The following special considerations in patients with chronic liver disease are reviewed: bone diseases in patients who underwent a liver transplant, the association between chronic hepatitis B virus infection treatment and bone diseases, the association between sarcopenia and bone diseases in patients with chronic liver disease, and the association between chronic liver disease and avascular necrosis of the hip. Few guidelines are currently available for the management of low bone mineral density or bone diseases in patients with chronic liver disease. Due to increased life expectancy and therapeutic advances in chronic liver disease, the importance of managing osteoporosis and other bone diseases in patients with chronic liver disease is expected to increase. Consequently, specific guidelines need to be established in the near future.
Keywords: biliary cholangitis; dysbiosis; liver cirrhosis; liver disease; liver transplantation; osteoporosis; sarcopenia; tenofovir disoproxil fumarate.
Conflict of interest statement
None of the authors have potential conflicts of interest to be disclosed.
Figures
References
-
- Burra P., Burroughsy A., Graziadei I., Pirenne J., Valdecasas J.C., Muiesan P., Samuel D., Forn X. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016;64:433–485. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
