

Antibacterial resistance in ophthalmic infections: a multi-centre analysis across UK care settings
- PMID: 31481023
- PMCID: PMC6724305
- DOI: 10.1186/s12879-019-4418-0
Antibacterial resistance in ophthalmic infections: a multi-centre analysis across UK care settings
Abstract
Background: Bacterial ophthalmic infections are common. Empirical treatment with topical broad-spectrum antibiotics is recommended for severe cases. Antimicrobial resistance (AMR) to agents used for bacterial ophthalmic infections make it increasingly important to consider changing resistance patterns when prescribing, however UK data in this area are lacking. We evaluate the epidemiology and antimicrobial susceptibilities of ophthalmic pathogens across care settings and compare these with local and national antimicrobial prescribing guidelines.
Methods: A retrospective, multi-centre observational analysis was undertaken of ophthalmic microbiology isolates between 2009 and 2015 at a centralised North-West London laboratory (incorporating data from primary care and five London teaching hospitals). Data were analysed using descriptive statistics with respect to patient demographics, pathogen distribution (across age-groups and care setting), seasonality, and susceptibility to topical chloramphenicol, moxifloxacin, and fusidic acid.
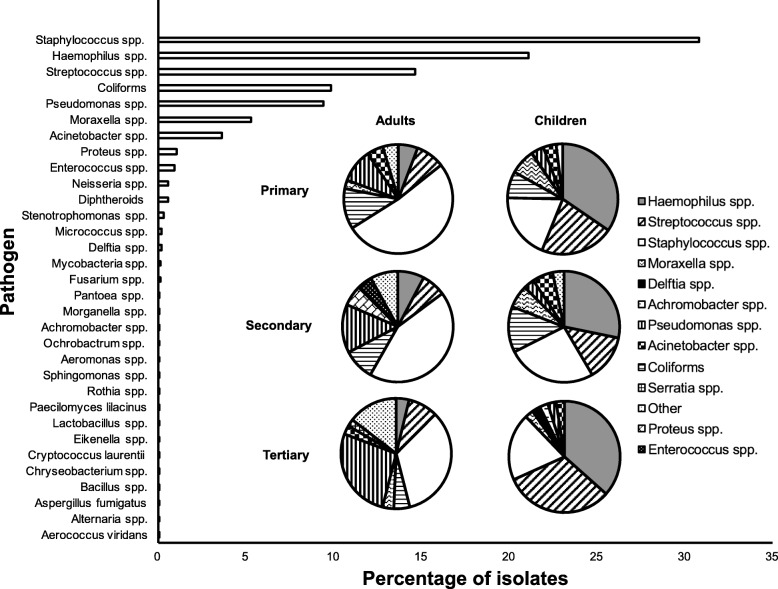
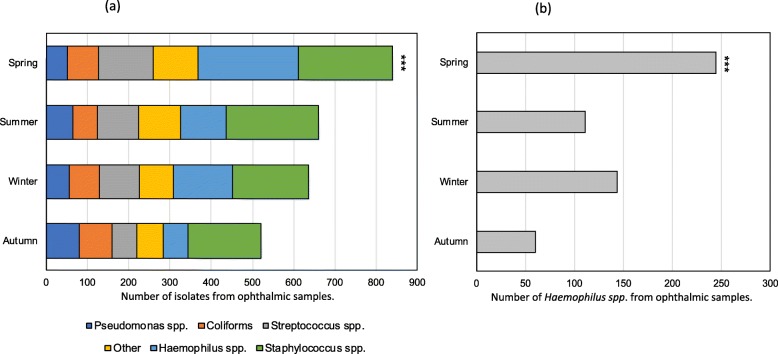
Results: Two thousand six hundred eighty-one isolates (n = 2168 patients) were identified. The commonest pathogen in adults was Staphylococcus spp. across primary, secondary, and tertiary care (51.7%; 43.4%; 33.6% respectively) and in children was Haemophilus spp. (34.6%;28.2%;36.6%). AMR was high and increased across care settings for chloramphenicol (11.8%;15.1%;33.8%); moxifloxacin (5.5%;7.6%;25.5%); and fusidic acid (49.6%;53.4%; 58.7%). Pseudomonas spp. was the commonest chloramphenicol-resistant pathogen across all care settings, whilst Haemophilus spp. was the commonest fusidic acid-resistant pathogen across primary and secondary care. More isolates were recorded in spring (31.6%) than any other season, mostly due to a significant rise in Haemophilus spp.
Conclusions: We find UK national and local antimicrobial prescribing policies for ophthalmic infections may not be concordant with the organisms and antimicrobial susceptibilities found in clinical samples. We also find variations in microbial incidence related to patient age, clinical setting, and season. Such variations may have further important implications for prescribing practices and modification of antimicrobial guidelines.
Keywords: Antimicrobial resistance; Antimicrobial stewardship; Conjunctivitis; Eye infections; Infectious diseases; Microbiology; Ophthalmology; Topical antimicrobials.
Conflict of interest statement
LSPM has consulted for bioMerieux (2013), DNAelectronics (2015–2018), Dairy Crest (2017–2018), received speaker fees from Profile Pharma (2018) and Pfizer (2018–2019), received research grants from the National Institute for Health Research (2013–2018), Leo Pharma (2016), and CW+ Charity (2017–2019), and received educational support from Eumedica (2016–2017). All other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Bacterial etiology and antimicrobial resistance trends in ocular infections: A 30-year study, Turin area, Italy.Eur J Ophthalmol. 2021 Mar;31(2):405-414. doi: 10.1177/1120672119896419. Epub 2019 Dec 25. Eur J Ophthalmol. 2021. PMID: 31875683
-
12-year analysis of incidence, microbiological profiles and in vitro antimicrobial susceptibility of infectious keratitis: the Nottingham Infectious Keratitis Study.Br J Ophthalmol. 2021 Mar;105(3):328-333. doi: 10.1136/bjophthalmol-2020-316128. Epub 2020 Jun 24. Br J Ophthalmol. 2021. PMID: 32580955 Free PMC article.
-
Bacteriological profile and drug susceptibility patterns in dacryocystitis patients attending Gondar University Teaching Hospital, Northwest Ethiopia.BMC Ophthalmol. 2015 Apr 2;15:34. doi: 10.1186/s12886-015-0016-0. BMC Ophthalmol. 2015. PMID: 25880996 Free PMC article.
-
Emerging antimicrobial resistance and need for antimicrobial stewardship for ocular infections in India: A narrative review.Indian J Ophthalmol. 2022 May;70(5):1513-1521. doi: 10.4103/ijo.IJO_2537_21. Indian J Ophthalmol. 2022. PMID: 35502016 Free PMC article. Review.
-
Trends in the Microbiological Spectrum of Nonviral Keratitis at a Single Tertiary Care Ophthalmic Hospital in India: A Review of 30 years.Cornea. 2023 Jul 1;42(7):837-846. doi: 10.1097/ICO.0000000000003105. Epub 2022 Jul 28. Cornea. 2023. PMID: 35942533 Review.
Cited by
-
Clinical characteristics of external bacterial ocular and periocular infections and their antimicrobial treatment patterns among a Ghanaian ophthalmic population.Sci Rep. 2022 Jun 17;12(1):10264. doi: 10.1038/s41598-022-14461-x. Sci Rep. 2022. PMID: 35715500 Free PMC article.
-
Effect of low dose honey on the apoptosis and inflammation gene expression in corneal limbal stem cells and keratocytes and its efficacy as an ophthalmic formulation in the treatment of dry eye: in-vitro and clinical study.Front Med (Lausanne). 2024 May 20;11:1359463. doi: 10.3389/fmed.2024.1359463. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38831993 Free PMC article.
-
The ocular surface bacterial contamination and its management in the prophylaxis of post cataract surgery endophthalmitis.Rom J Ophthalmol. 2021 Jan-Mar;65(1):2-9. doi: 10.22336/rjo.2021.2. Rom J Ophthalmol. 2021. PMID: 33817426 Free PMC article. Review.
-
Conjunctival sac flora and drug susceptibility analysis in normal children in East China.BMC Ophthalmol. 2023 Jun 2;23(1):248. doi: 10.1186/s12886-023-02995-1. BMC Ophthalmol. 2023. PMID: 37268920 Free PMC article.
-
Ozonated Oil in Liposome Eyedrops Reduces the Formation of Biofilm, Selection of Antibiotic-Resistant Bacteria, and Adhesion of Bacteria to Human Corneal Cells.Int J Mol Sci. 2023 Sep 14;24(18):14078. doi: 10.3390/ijms241814078. Int J Mol Sci. 2023. PMID: 37762377 Free PMC article.
References
-
- Antimicrobial resistance: global report on surveillance [Internet]. World Health Organisation. 2014 [cited 2018 Jan 17]. Available from: http://apps.who.int/iris/bitstream/10665/112642/1/9789241564748_eng.pdf?....
-
- Freeman R, Moore LSP, Charlett A, Donaldson H, Holmes AH. Exploring the epidemiology of carbapenem-resistant gram-negative bacteria in West London and the utility of routinely collected hospital microbiology data. J Antimicrob Chemother. 2014;70(4):1212–1218. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
