

Efficacy and safety of 1C class antiarrhythmic agent (propafenone) for supraventricular arrhythmias in septic shock compared to amiodarone: protocol of a prospective randomised double-blind study
- PMID: 31481571
- PMCID: PMC6731952
- DOI: 10.1136/bmjopen-2019-031678
Efficacy and safety of 1C class antiarrhythmic agent (propafenone) for supraventricular arrhythmias in septic shock compared to amiodarone: protocol of a prospective randomised double-blind study
Abstract
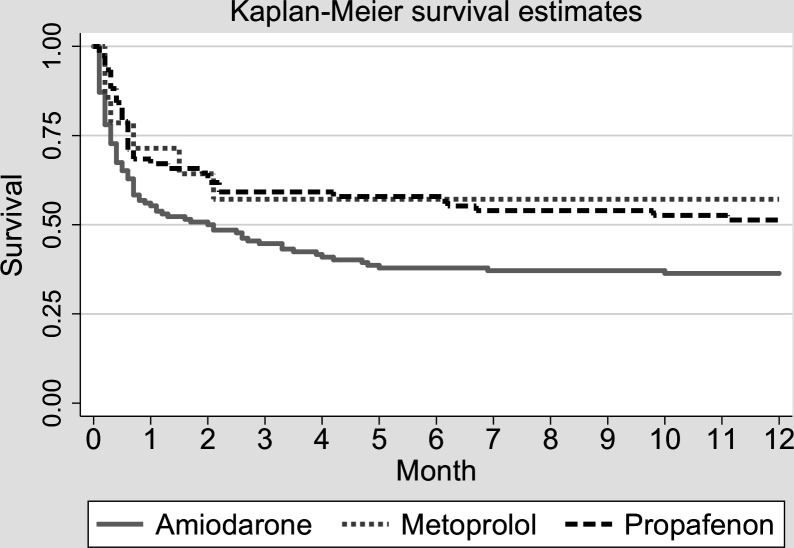
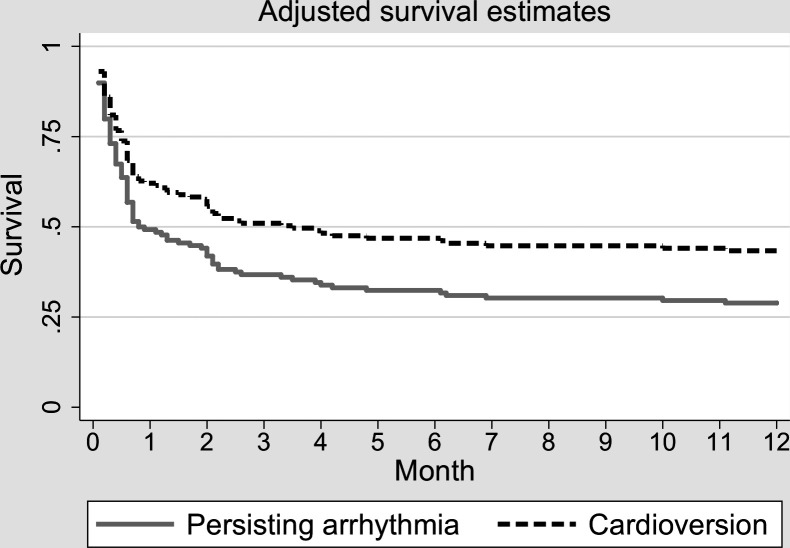
Introduction: Supraventricular arrhythmias contribute to haemodynamic compromise in septic shock. A retrospective study generated the hypothesis that propafenone could be more effective than amiodarone in achieving and maintaining sinus rhythm (SR). Certain echocardiographic parameters may predict a successful cardioversion and help in the decision on rhythm or rate control strategy.
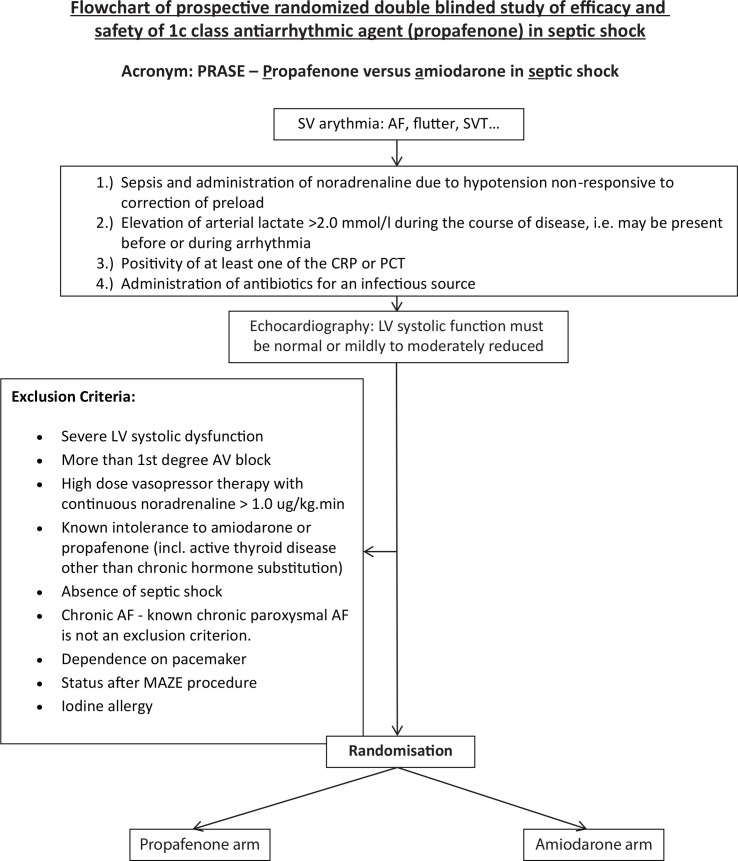
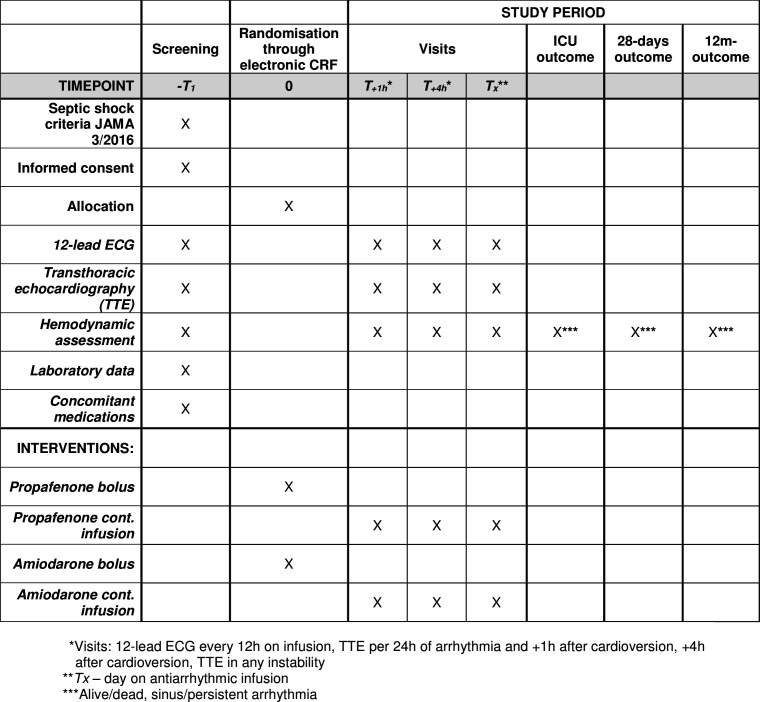
Methods and analysis: The trial includes septic shock patients with new-onset arrhythmia, but without severe impairment of the left ventricular ejection fraction. After baseline echocardiography, the patient is randomised to receive a bolus and maintenance dose of either amiodarone or propafenone. The primary outcome is the proportion of patients that have achieved rhythm control at 24 hours after the start of the infusion. The secondary outcomes are the percentages of patients that needed rescue treatments (DC cardioversion or unblinding and crossover of the antiarrhythmics), the recurrence of arrhythmias, intensive care unit mortality, 28-day and 1-year mortality. In the posthoc analysis, we separately assess subgroups of patients with pulmonary hypertension and right ventricular dysfunction. In the exploratory part of the study, we assess whether the presence of a transmitral diastolic A wave and its higher velocity-time integral is predictive for the sustainability of mechanical SR and whether the indexed left atrial endsystolic volume is predictive of recurrent arrhythmia. Considering that the restoration of SR within 24 hours occurred in 74% of the amiodarone-treated patients and in 89% of the patients treated with propafenone, we plan to include 200 patients to have an 80% chance to demonstrate the superiority of propafenone at p=0.05.
Ethics and dissemination: The trial is recruiting patients according to its second protocol version approved by the University Hospital Ethical Board on the 6 October 2017 (No. 1691/16S-IV). The results will be disseminated through peer reviewed publications and conference presentations.
Trial registration number: NCT03029169.
Keywords: amiodarone; intensive care; propafenone; septic shock; supraventricular arrhythmia.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials