

Supplemental Oxygen for Treatment of Infants With Obstructive Sleep Apnea
- PMID: 31482833
- PMCID: PMC6707057
- DOI: 10.5664/jcsm.7802
Supplemental Oxygen for Treatment of Infants With Obstructive Sleep Apnea
Abstract
Study objectives: Supplemental oxygen has been shown to decrease the frequency of obstructive respiratory events during sleep, but may result in alveolar hypoventilation. Limited information exists on the effect of supplemental oxygen on sleep and respiratory events in infants with obstructive sleep apnea (OSA).
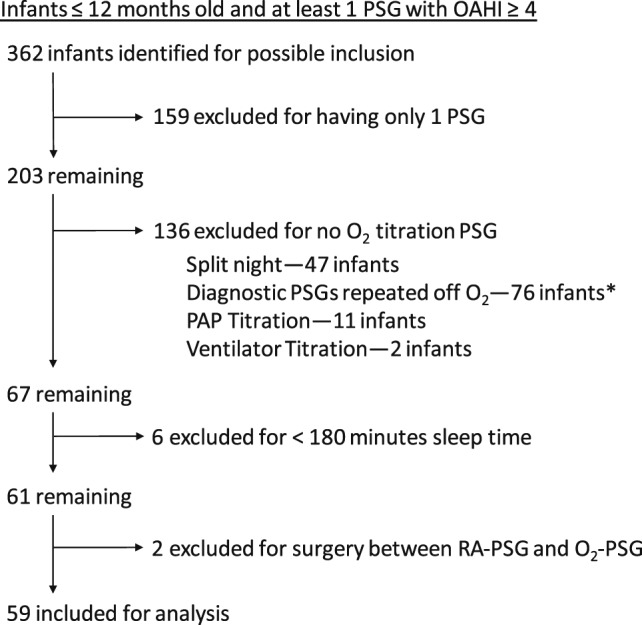
Methods: We conducted a retrospective study of infants with OSA who had sleep studies performed from 2007-2012. All infants underwent a room air diagnostic sleep study (RA-PSG), followed by a sleep study while breathing supplemental oxygen via nasal cannula (O₂-PSG) on a separate night. Infants with split-night studies or with inadequate sleep time were excluded.
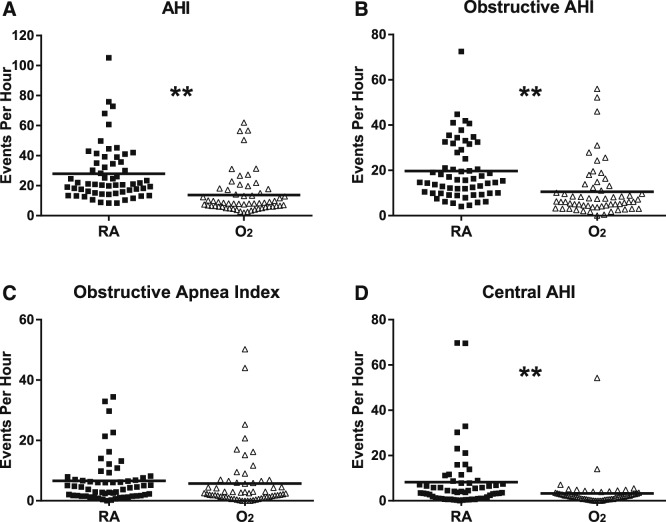
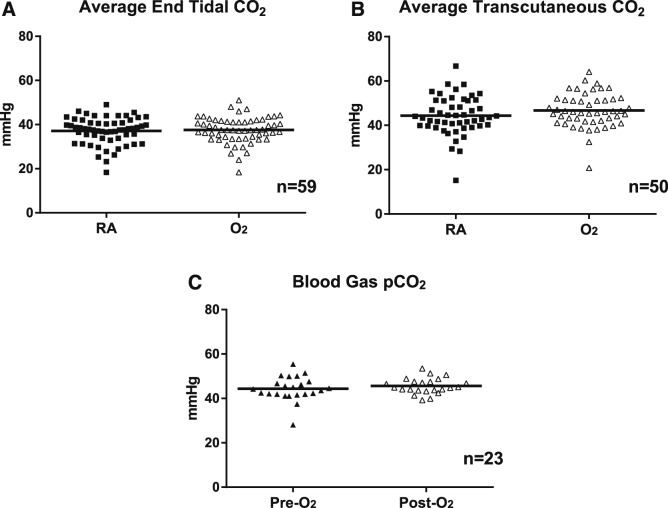
Results: Fifty-nine infants met criteria for entry into analysis. The mean age of infants at the time of RA-PSG was 13.0 ± 11.7 weeks and at O₂-PSG was 15.4 ± 13.0 weeks. The obstructive AHI decreased from 19.7 ± 13.0 during RA-PSG to 10.6 ± 11.7 during O₂-PSG (P < .001). The duration of longest obstructive apnea increased from 11.0 ± 4.2 seconds to 13.4 ± 7.4 seconds (P = .01). The lowest saturation associated with obstructive apneas increased from 80.7 ± 6.8% to 90.0 ± 6.7% (P < .001). Carbon dioxide data showed no difference in ventilation after supplemental oxygen administration. There was no significant change in the spontaneous arousal index, however, the percentage of respiratory events associated with arousal increased from 20.7 ± 11.1% to 35.7 ± 19.7% (P < .001).
Conclusions: Infants with OSA who received supplemental oxygen had a significant decrease in the frequency of obstructive respiratory events and improved oxygenation without adverse effect on alveolar ventilation. These data suggest that supplemental oxygen may be an effective treatment for infants with OSA who are not good candidates for continuous positive airway pressure or surgery.
Citation: Brockbank J, Astudillo CL, Che D, Tanphaichitr A, Huang G, Tomko J, Simakajornboon N. Supplemental oxygen for treatment of infants with obstructive sleep apnea. J Clin Sleep Med. 2019;15(8):1115-1123.
Keywords: infant sleep; oxygen therapy; pediatric OSA; respiratory control.
© 2019 American Academy of Sleep Medicine.
Figures
References
-
- Gozal D. Sleep, sleep disorders and inflammation in children. Sleep Med. 2009;10(Suppl 1):S12–S16. - PubMed
-
- Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: association with race and prematurity. J Pediatr. 2003;142(4):383–389. - PubMed
-
- Gislason T, Benediktsdottir B. Snoring, apneic episodes, and nocturnal hypoxemia among children 6 months to 6 years old. An epidemiologic study of lower limit of prevalence. Chest. 1995;107(4):963–966. - PubMed
-
- Anuntaseree W, Kuasirikul S, Suntornlohanakul S. Natural history of snoring and obstructive sleep apnea in Thai school-age children. Pediatr Pulmonol. 2005;39(5):415–420. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
