

Hypertensive crisis: clinical characteristics of patients with hypertensive urgency, emergency and pseudocrisis at a public emergency department
- PMID: 31482942
- PMCID: PMC6711750
- DOI: 10.31744/einstein_journal/2019AO4685
Hypertensive crisis: clinical characteristics of patients with hypertensive urgency, emergency and pseudocrisis at a public emergency department
Abstract
Objective: To assess patients with hypertensive crisis, classified as urgency, emergency or pseudocrisis, and identify the associated variables.
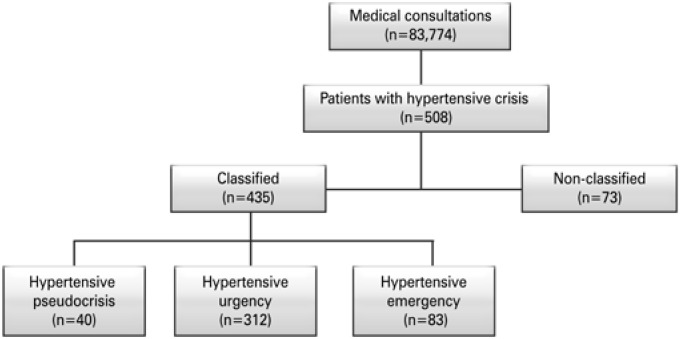
Methods: We evaluated a total of 508 patients (57% women; 56.3±13.8 years old) with hypertensive crisis (diastolic blood pressure of 120mmHg), aged 18 years or over, seen at the emergency department of a public general hospital.
Results: The prevalence of hypertensive crises was 6/1,000; in that, 71.7% presented hypertensive urgency, 19.1% hypertensive emergency, and 9.2% hypertensive pseudocrisis. In the multinominal logistic regression, pseudocrisis and urgency conditions were compared to hypertensive emergency. Therefore, the presence of pain (OR: 55.58; 95%CI: 10.55-292.74) except chest pain and headache, and emotional problems (OR: 17.13; 95%CI: 2.80-104.87) increased the likelihood of hypertensive pseudocrisis. Age >60 years (OR: 0,32; 95%CI: 0.10-0.96) and neurologic problems (OR: 1.5.10-8; 95%CI: 1.5.10-8-1.5.10-8) protected against hypertensive pseudocrisis. The comparison of hypertensive urgency with hypertensive emergency showed that age >60 years (OR: 0.50; 95%CI: 0.27-0.92), neurologic (OR: 0.09; 95%CI: 0.04-0.18) and emotional problems (OR: 0.06; 95%CI: 4.7.10-3-0.79) protected against hypertensive urgency. Moreover, only headache (OR: 14.28; 95%CI: 3.32-61.47) increased the likelihood of hypertensive urgency.
Conclusion: Advanced age and neurological problems were associated to hypertensive emergency. Headache was associated with hypertensive urgency. Pain and emotional problems were associated with hypertensive pseudocrisis. Our results can contribute to identifying patients with hypertensive crisis who seek emergency services.
Objetivo:: Avaliar pacientes com crise hipertensiva, classificada em urgência, emergência ou pseudocrise, e identificar variáveis associadas.
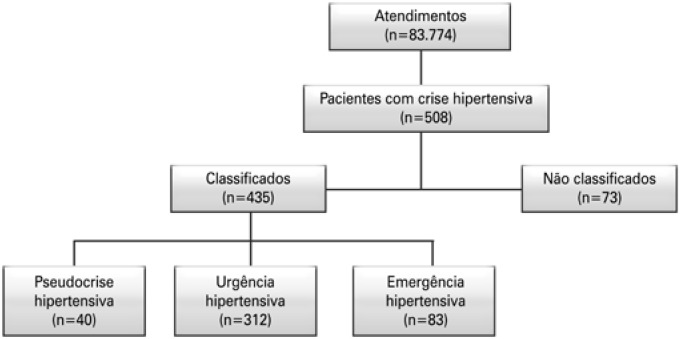
Métodos:: Foram avaliados 508 pacientes (57% mulheres; 56,3±13,8 anos) com crise hipertensiva (pressão diastólica de 120mmHg), idade maior ou igual a 18 anos, atendidos em um serviço de emergência de um hospital geral público. A crise hipertensiva foi classificada em urgência, emergência ou pseudocrise.
Resultados:: A prevalência da crise hipertensiva foi 6/1.000, com 71,7% com urgência hipertensiva, 19,1% com emergência hipertensiva e 9,2% com pseudocrise hipertensiva. Na análise de regressão logística multinomial, as condições de pseudocrise e urgência foram comparadas com a emergência hipertensiva. Assim, presença de dor (OR: 55,58; IC95%: 10,55-292,74), exceto precordialgia e cefaleia, e problemas emocionais (OR: 17,13; IC95%: 2,80-104,87) elevaram a chance para pseudocrise hipertensiva. Idade acima de 60 anos (OR: 0,32; IC95%: 0,10-0,96) e problemas neurológicos (OR: 1,5.10-8; IC95%: 1,5.10-8-1,5.10-8) foram protetores para pseudocrise hipertensiva. A urgência hipertensiva comparada com emergência hipertensiva mostrou que idade acima de 60 anos (OR: 0,50; IC95%: 0,27-0,92), problemas neurológicos (OR: 0,09; IC95%: 0,04-0,18) e emocionais (OR: 0,06; IC95%: 4,7.10-3-0,79) foram protetores para urgência hipertensiva, e apenas cefaleia (OR: 14,28; IC95%: 3,32-61,47) elevou a chance para urgência hipertensiva.
Conclusão:: Idade mais elevada e problemas neurológicos se associaram à emergência hipertensiva. Cefaleia associou-se à urgência hipertensiva. Dor e problemas emocionais se associaram à pseudocrise hipertensiva. Nossos resultados podem contribuir para aprimorar a identificação de pacientes com crise hipertensiva que procuram serviços de emergência.
Conflict of interest statement
Figures
Similar articles
-
Occurrence rate and clinical predictors of hypertensive pseudocrisis in emergency room care.Arq Bras Cardiol. 2007 May;88(5):579-84. doi: 10.1590/s0066-782x2007000500013. Arq Bras Cardiol. 2007. PMID: 17589634 English, Portuguese.
-
Profile of patients with hypertensive urgency and emergency presenting to an urban emergency department of a tertiary referral hospital in Tanzania.BMC Cardiovasc Disord. 2018 Aug 2;18(1):158. doi: 10.1186/s12872-018-0895-0. BMC Cardiovasc Disord. 2018. PMID: 30068315 Free PMC article.
-
[Prevalence and severity of hypertensive emergencies and outbreaks in the hospital emergency department of CHU Timone at Marseille: Follow-up in three months of hospitalized patients].Ann Cardiol Angeiol (Paris). 2016 Jun;65(3):185-90. doi: 10.1016/j.ancard.2016.04.005. Epub 2016 May 13. Ann Cardiol Angeiol (Paris). 2016. PMID: 27184512 French.
-
Risk factors for hypertensive crisis in adult patients: a systematic review.JBI Evid Synth. 2021 Jun;19(6):1292-1327. doi: 10.11124/JBIES-20-00243. JBI Evid Synth. 2021. PMID: 33555818
-
Evaluation and management of pediatric hypertensive crises: hypertensive urgency and hypertensive emergencies.Open Access Emerg Med. 2012 Sep 5;4:85-92. doi: 10.2147/OAEM.S32809. eCollection 2012. Open Access Emerg Med. 2012. PMID: 27147865 Free PMC article. Review.
Cited by
-
Brazilian Guidelines of Hypertension - 2020.Arq Bras Cardiol. 2021 Mar;116(3):516-658. doi: 10.36660/abc.20201238. Arq Bras Cardiol. 2021. PMID: 33909761 Free PMC article. English, Portuguese. No abstract available.
-
Assessing the impact of acute severe hypertension in the emergency department: A prospective cohort study in Karachi, Pakistan.PLOS Glob Public Health. 2024 Dec 4;4(12):e0003948. doi: 10.1371/journal.pgph.0003948. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39630660 Free PMC article.
-
Proposal of a Modified Classification of Hypertensive Crises: Urgency, Impending Emergency, and Emergency.Curr Vasc Pharmacol. 2024;22(3):180-186. doi: 10.2174/0115701611270174231204110557. Curr Vasc Pharmacol. 2024. PMID: 39188222 Review.
-
Clinico-epidemiological profile and risk factors of hypertensive crisis among patients attended at a tertiary care hospital in Somalia.Sci Rep. 2023 Jan 9;13(1):447. doi: 10.1038/s41598-023-27683-4. Sci Rep. 2023. PMID: 36624249 Free PMC article.
-
Cost effectiveness of mono, dual, and triple therapy of antihypertensive drugs: a retrospective cohort study.Cost Eff Resour Alloc. 2025 Aug 14;23(1):43. doi: 10.1186/s12962-025-00614-y. Cost Eff Resour Alloc. 2025. PMID: 40813675 Free PMC article.
References
-
- World Health Organization (WHO) A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis [Internet] Geneva: WHO; 2013. [[cited 2018 Sep 2018]]. Available from: http://www.who.int/cardiovascular_diseases/publications/global_brief_hyp....
- 1. World Health Organization (WHO). A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis [Internet]. Geneva: WHO; 2013 [cited 2018 Sep 2018]. Available from: http://www.who.int/cardiovascular_diseases/publications/global_brief_hyp....
-
- Muiesan ML, Salvetti M, Amadoro V, di Somma S, Perlini S, Semplicini A, Borghi C, Volpe M, Saba PS, Cameli M, Ciccone MM, Maiello M, Modesti PA, Novo S, Palmiero P, Scicchitano P, Rosei EA, Pedrinelli R. Working Group on Hypertension, Prevention, Rehabilitation of the Italian Society of Cardiology, the Societa' Italiana dell'Ipertensione Arteriosa. An update on hypertensive emergencies and urgencies. J Cardiovasc Med (Hagerstown) 2015;16(5):372–382. Review. - PubMed
- 3. Muiesan ML, Salvetti M, Amadoro V, di Somma S, Perlini S, Semplicini A, Borghi C, Volpe M, Saba PS, Cameli M, Ciccone MM, Maiello M, Modesti PA, Novo S, Palmiero P, Scicchitano P, Rosei EA, Pedrinelli R; Working Group on Hypertension, Prevention, Rehabilitation of the Italian Society of Cardiology, the Societa' Italiana dell'Ipertensione Arteriosa. An update on hypertensive emergencies and urgencies. J Cardiovasc Med (Hagerstown). 2015;16(5):372-82. Review. - PubMed
-
- Ipek E, Oktay AA, Krim SR. Hypertensive crisis: an update on clinical approach and management. Curr Opin Cardiol. 2017;32(4):397–406. Review. - PubMed
- 4. Ipek E, Oktay AA, Krim SR. Hypertensive crisis: an update on clinical approach and management. Curr Opin Cardiol. 2017;32(4):397-406. Review. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. Erratum in: JAMA. 2003;290(2):197. - PubMed
- 5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560-72. Erratum in: JAMA. 2003;290(2):197. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
