Genetic hallmarks of recurrent/metastatic adenoid cystic carcinoma
- PMID: 31483290
- PMCID: PMC6763222
- DOI: 10.1172/JCI128227
Genetic hallmarks of recurrent/metastatic adenoid cystic carcinoma
Abstract
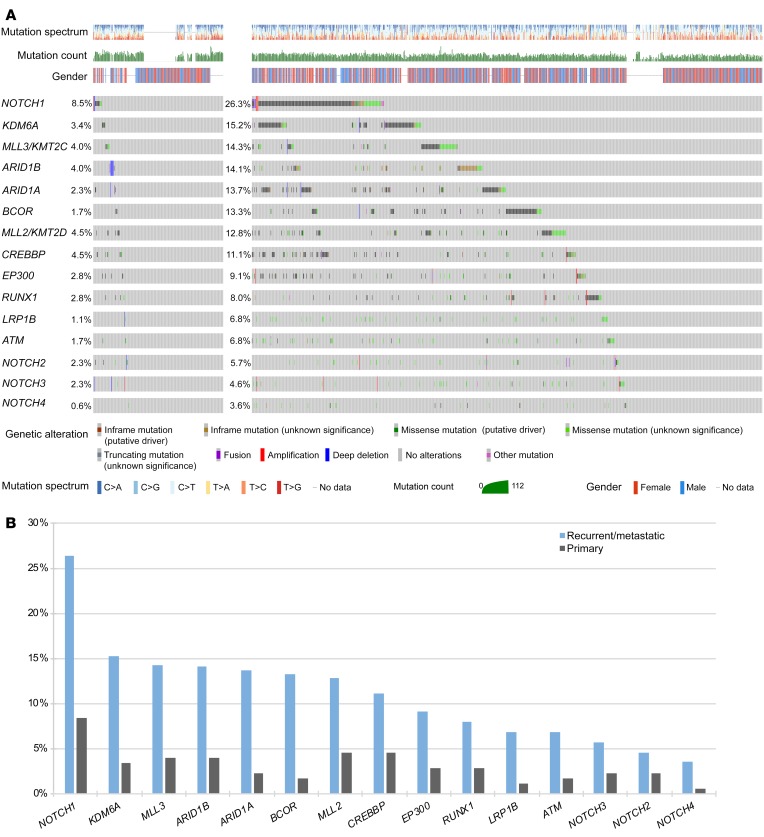
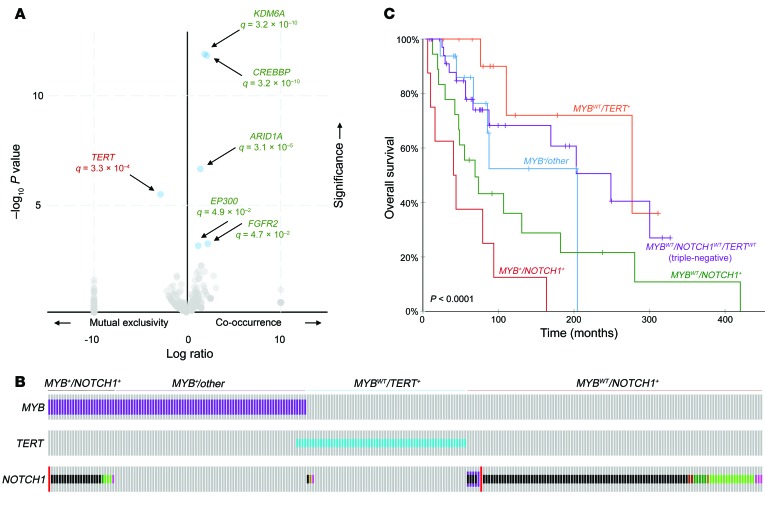
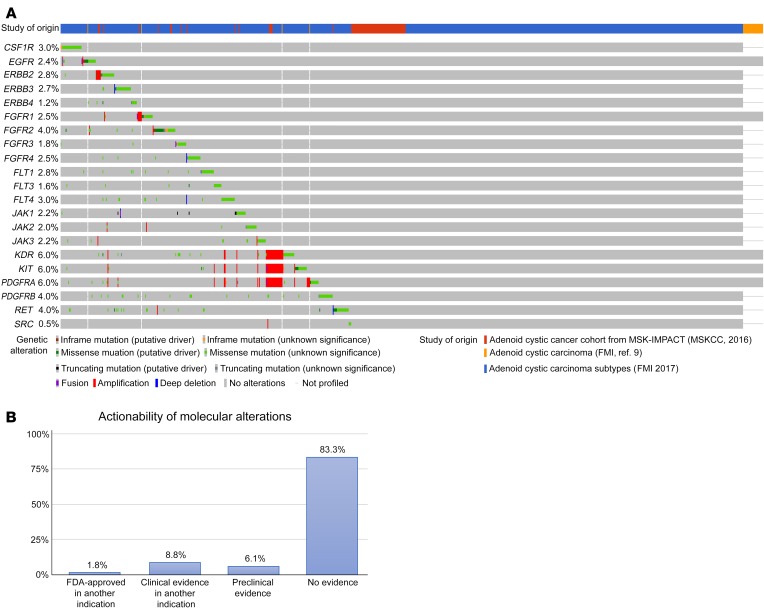
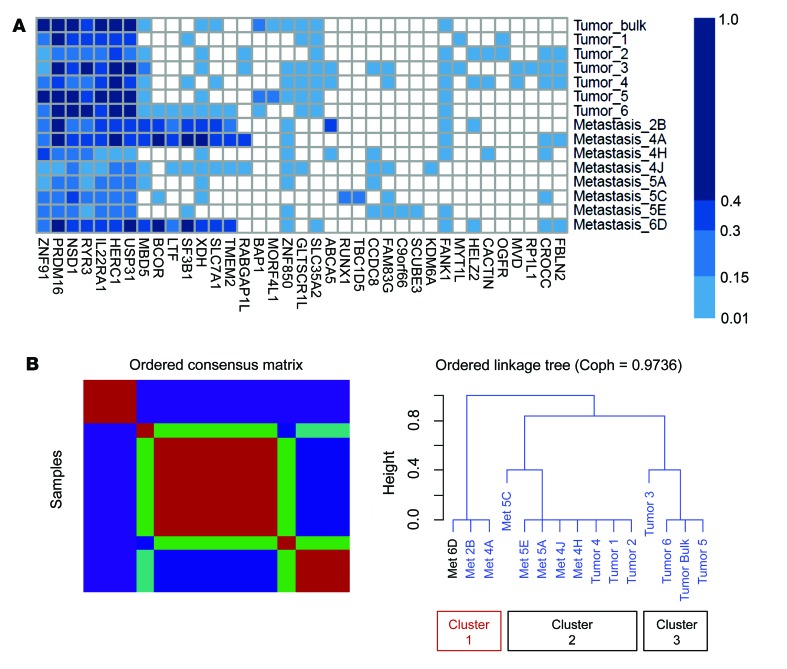
BACKGROUNDAdenoid cystic carcinoma (ACC) is a rare malignancy arising in salivary glands and other sites, characterized by high rates of relapse and distant spread. Recurrent/metastatic (R/M) ACCs are generally incurable, due to a lack of active systemic therapies. To improve outcomes, deeper understanding of genetic alterations and vulnerabilities in R/M tumors is needed.METHODSAn integrated genomic analysis of 1,045 ACCs (177 primary, 868 R/M) was performed to identify alterations associated with advanced and metastatic tumors. Intratumoral genetic heterogeneity, germline mutations, and therapeutic actionability were assessed.RESULTSCompared with primary tumors, R/M tumors were enriched for alterations in key Notch (NOTCH1, 26.3% vs. 8.5%; NOTCH2, 4.6% vs. 2.3%; NOTCH3, 5.7% vs. 2.3%; NOTCH4, 3.6% vs. 0.6%) and chromatin-remodeling (KDM6A, 15.2% vs. 3.4%; KMT2C/MLL3, 14.3% vs. 4.0%; ARID1B, 14.1% vs. 4.0%) genes. TERT promoter mutations (13.1% of R/M cases) were mutually exclusive with both NOTCH1 mutations (q = 3.3 × 10-4) and MYB/MYBL1 fusions (q = 5.6 × 10-3), suggesting discrete, alternative mechanisms of tumorigenesis. This network of alterations defined 4 distinct ACC subgroups: MYB+NOTCH1+, MYB+/other, MYBWTNOTCH1+, and MYBWTTERT+. Despite low mutational load, we identified numerous samples with marked intratumoral genetic heterogeneity, including branching evolution across multiregion sequencing.CONCLUSIONThese observations collectively redefine the molecular underpinnings of ACC progression and identify further targets for precision therapies.FUNDINGAdenoid Cystic Carcinoma Research Foundation, Pershing Square Sohn Cancer Research grant, the PaineWebber Chair, Stand Up 2 Cancer, NIH R01 CA205426, the STARR Cancer Consortium, NCI R35 CA232097, the Frederick Adler Chair, Cycle for Survival, the Jayme Flowers Fund, The Sebastian Nativo Fund, NIH K08 DE024774 and R01 DE027738, and MSKCC through NIH/NCI Cancer Center Support Grant (P30 CA008748).
Keywords: Head and neck cancer; Oncology.
Conflict of interest statement
Figures