

Patterns of Recurrence After Resection of Pancreatic Ductal Adenocarcinoma: A Secondary Analysis of the ESPAC-4 Randomized Adjuvant Chemotherapy Trial
- PMID: 31483448
- PMCID: PMC6727687
- DOI: 10.1001/jamasurg.2019.3337
Patterns of Recurrence After Resection of Pancreatic Ductal Adenocarcinoma: A Secondary Analysis of the ESPAC-4 Randomized Adjuvant Chemotherapy Trial
Abstract
Importance: The patterns of disease recurrence after resection of pancreatic ductal adenocarcinoma with adjuvant chemotherapy remain unclear.
Objective: To define patterns of recurrence after adjuvant chemotherapy and the association with survival.
Design, setting, and participants: Prospectively collected data from the phase 3 European Study Group for Pancreatic Cancer 4 adjuvant clinical trial, an international multicenter study. The study included 730 patients who had resection and adjuvant chemotherapy for pancreatic cancer. Data were analyzed between July 2017 and May 2019.
Interventions: Randomization to adjuvant gemcitabine or gemcitabine plus capecitabine.
Main outcomes and measures: Overall survival, recurrence, and sites of recurrence.
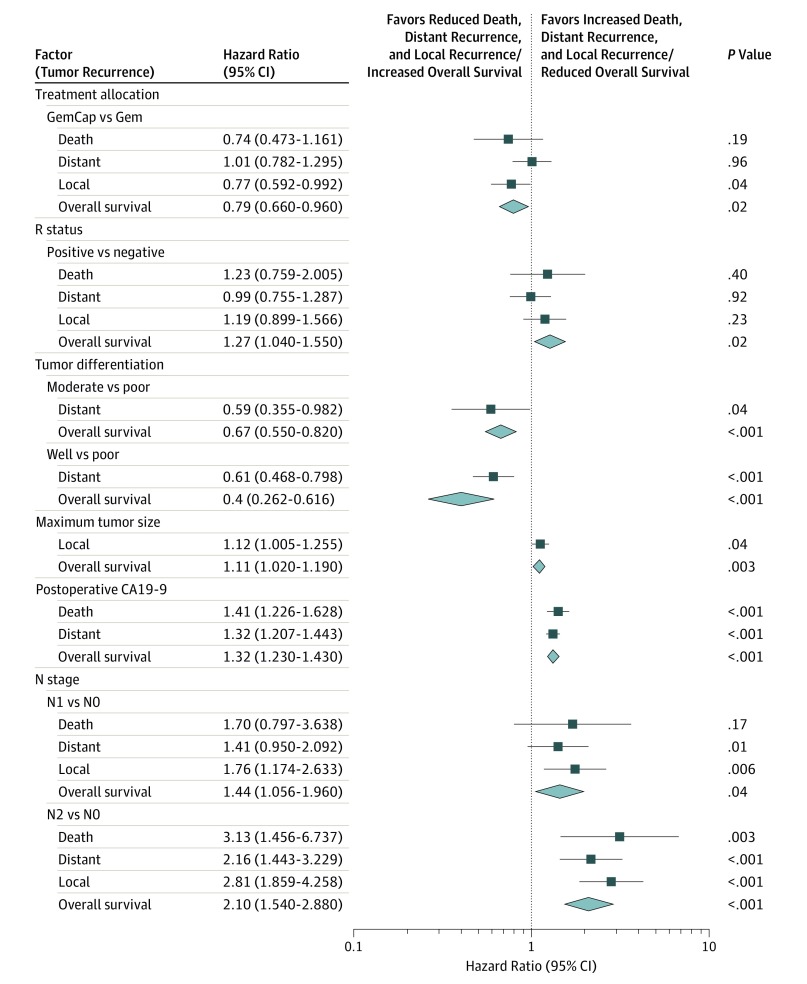
Results: Of the 730 patients, median age was 65 years (range 37-81 years), 414 were men (57%), and 316 were women (43%). The median follow-up time from randomization was 43.2 months (95% CI, 39.7-45.5 months), with overall survival from time of surgery of 27.9 months (95% CI, 24.8-29.9 months) with gemcitabine and 30.2 months (95% CI, 25.8-33.5 months) with the combination (HR, 0.81; 95% CI, 0.68-0.98; P = .03). The 5-year survival estimates were 17.1% (95% CI, 11.6%-23.5%) and 28.0% (22.0%-34.3%), respectively. Recurrence occurred in 479 patients (65.6%); another 78 patients (10.7%) died without recurrence. Local recurrence occurred at a median of 11.63 months (95% CI, 10.05-12.19 months), significantly different from those with distant recurrence with a median of 9.49 months (95% CI, 8.44-10.71 months) (HR, 1.21; 95% CI, 1.01-1.45; P = .04). Following recurrence, the median survival was 9.36 months (95% CI, 8.08-10.48 months) for local recurrence and 8.94 months (95% CI, 7.82-11.17 months) with distant recurrence (HR, 0.89; 95% CI, 0.73-1.09; P = .27). The median overall survival of patients with distant-only recurrence (23.03 months; 95% CI, 19.55-25.85 months) or local with distant recurrence (23.82 months; 95% CI, 17.48-28.32 months) was not significantly different from those with only local recurrence (24.83 months; 95% CI, 22.96-27.63 months) (P = .85 and P = .35, respectively). Gemcitabine plus capecitabine had a 21% reduction of death following recurrence compared with monotherapy (HR, 0.79; 95% CI, 0.64-0.98; P = .03).
Conclusions and relevance: There were no significant differences between the time to recurrence and subsequent and overall survival between local and distant recurrence. Pancreatic cancer behaves as a systemic disease requiring effective systemic therapy after resection.
Trial registration: ClinicalTrials.gov identifier: NCT00058201, EudraCT 2007-004299-38, and ISRCTN 96397434.
Conflict of interest statement
Figures


Comment in
-
Pancreatic Ductal Adenocarcinoma-ESPAC…or It's Back?JAMA Surg. 2019 Nov 1;154(11):1048. doi: 10.1001/jamasurg.2019.3364. JAMA Surg. 2019. PMID: 31483455 No abstract available.
-
Recurrence After Resection of Pancreatic Ductal Adenocarcinoma.JAMA Surg. 2020 Apr 1;155(4):361-362. doi: 10.1001/jamasurg.2019.5464. JAMA Surg. 2020. PMID: 31895430 No abstract available.
-
Recurrence After Resection of Pancreatic Ductal Adenocarcinoma-Reply.JAMA Surg. 2020 Apr 1;155(4):362-363. doi: 10.1001/jamasurg.2019.5465. JAMA Surg. 2020. PMID: 31895438 No abstract available.
-
Gastrointestinal Cancers: Moving the Needle for Rectal, Gastroesophageal, Pancreaticobiliary, and Liver Cancers.Int J Radiat Oncol Biol Phys. 2020 Mar 15;106(4):653-662. doi: 10.1016/j.ijrobp.2019.12.011. Int J Radiat Oncol Biol Phys. 2020. PMID: 32092335 No abstract available.
