Association of Germline Variants in Natural Killer Cells With Tumor Immune Microenvironment Subtypes, Tumor-Infiltrating Lymphocytes, Immunotherapy Response, Clinical Outcomes, and Cancer Risk
- PMID: 31483464
- PMCID: PMC6727785
- DOI: 10.1001/jamanetworkopen.2019.9292
Association of Germline Variants in Natural Killer Cells With Tumor Immune Microenvironment Subtypes, Tumor-Infiltrating Lymphocytes, Immunotherapy Response, Clinical Outcomes, and Cancer Risk
Erratum in
-
Error in Methods.JAMA Netw Open. 2020 Apr 1;3(4):e206708. doi: 10.1001/jamanetworkopen.2020.6708. JAMA Netw Open. 2020. PMID: 32329767 Free PMC article. No abstract available.
Abstract
Importance: Only a small fraction of patients with cancer receiving immune checkpoint therapy (ICT) respond, which is associated with tumor immune microenvironment (TIME) subtypes and tumor-infiltrating lymphocytes (TILs).
Objective: To examine whether germline variants of natural killer (NK) cells, a key component of the immune system, are associated with TIME subtypes, the abundance of TILs, response to ICT, clinical outcomes, and cancer risk.
Design, setting, and participants: This genetic association study explored TIME subtypes and examined the association of the germline genomic information of patients with cancer with TIME subtypes, abundance of TILs, response to ICT, prognosis, and cancer risk. Clinical information, tumor RNA sequencing, and whole-exome sequencing (WES) data of paired normal samples of patients with 13 common cancers (n = 5883) were obtained from the Cancer Genome Atlas. The WES data of individuals with no cancer (n = 4500) were obtained from the database of Genotypes and Phenotypes. Data collection and analysis took place in March 2017.
Main outcomes and measures: Associations between the number of germline defective genes in NK cells and survival time and the abundance of TILs.
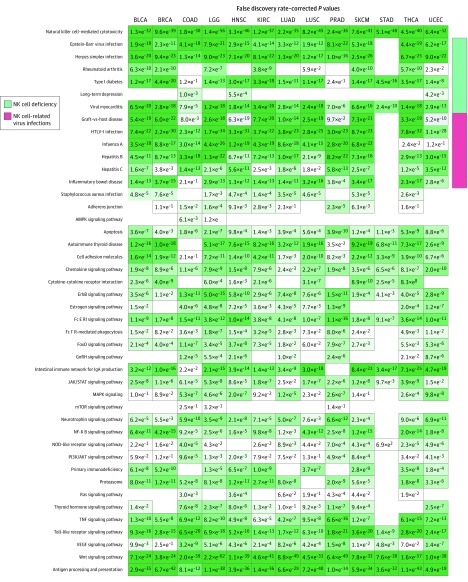
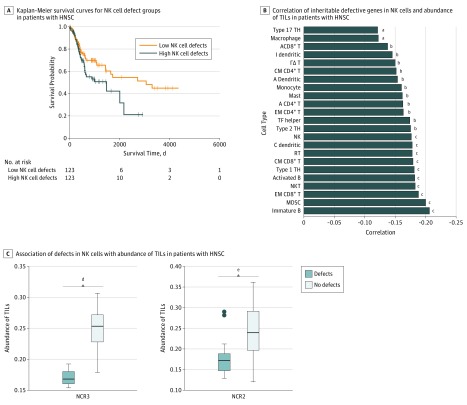
Results: Based on tumor RNA sequencing data, tumors were stratified into TIME-rich, TIME-intermediate, and TIME-poor subtypes. Tumors of TIME-rich subtype had more TILs (TIL-NK cells in TIME-rich head and neck squamous cell carcinoma [HNSC] tumors: t = 4.85; 95% CI of the difference, 0.01-0.03; P = 2.19 × 10-6) compared with TIME-intermediate HNSC tumors (t = 3.70; 95% CI of the difference, 0.01-0.03; P < .001), better prognosis (patients with HNSC: hazard ratio, 0.65; 95% CI, 0.41-1.02; P = .054) compared with TIME-intermediate and TIME-poor subtypes, and better ICT response (patients with melanoma: odds ratio [OR], 4.45; 95% CI, 0.99-27.08; P = .04). Patients with TIME-rich tumors had significantly fewer inherited defective genes in NK cells than patients with TIME-intermediate and TIME-poor tumors (patients with HNSC: OR, 0.49; 95% CI, 0.26-1.07; P = .005). Similarly, patients with cancer had significantly more inherited defective genes in NK cells than individuals with no cancer (patients with HNSC: OR, 19.09; 95% CI, 4.30-315.96; P = 6.21 × 10-4). Among 11 of 13 common cancers, the number of heritable defective genes in NK cells was significantly negatively associated with survival (patients with HNSC: hazard ratio, 1.77; 95% CI, 1.18-2.66; P = .005), abundance of TILs (patients with HNSC: R = -0.25; 95% CI, -0.65-2.17; P = 0.02), and response to ICT (patients with melanoma: OR, 4.45; 95% CI, 0.99-27.08; P = .04).
Conclusions and relevance: These results suggest that individuals who have more inherited defective genes in NK cells had a higher risk of developing cancer and that these inherited defects were associated with TIME subtypes, recruitment of TILs, ICT response, and clinical outcomes. The findings have implications for identifying individuals at risk for developing cancer of many types based on germline variants of NK cells and for improving existing ICT and chimeric antigen receptor-T cell therapy by adoptive transfer of healthy NK cells to patients with TIME-intermediate and TIME-poor tumors.
Conflict of interest statement
Figures