

Identification of Patients With High Mortality Risk and Prediction of Outcomes in Delirium by Bispectral EEG
- PMID: 31483958
- PMCID: PMC7181374
- DOI: 10.4088/JCP.19m12749
Identification of Patients With High Mortality Risk and Prediction of Outcomes in Delirium by Bispectral EEG
Abstract
Background: Delirium is common and dangerous, yet underdetected and undertreated. Current screening questionnaires are subjective and ineffectively implemented in busy hospital workflows. Electroencephalography (EEG) can objectively detect the diffuse slowing characteristic of delirium, but it is not suitable for high-throughput screening due to size, cost, and the expertise required for lead placement and interpretation. This study hypothesized that an efficient and reliable point-of-care EEG device for high-throughput screening could be developed.
Methods: This prospective study, which measured bispectral EEG (BSEEG) from elderly inpatients to assess their outcomes, was conducted at the University of Iowa Hospitals and Clinics from January 2016 to October 2017. A BSEEG score was defined based on the distribution of 2,938 EEG recordings from the 428 subjects who were assessed for delirium; primary outcomes measured were hospital length of stay, discharge disposition, and mortality.
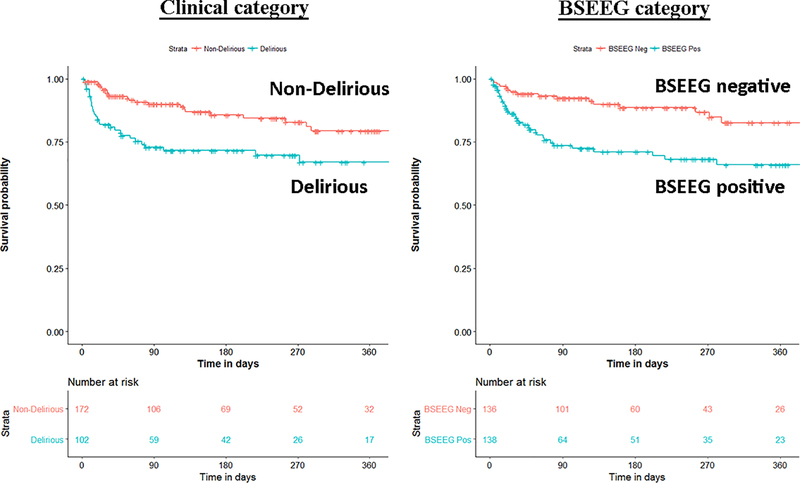
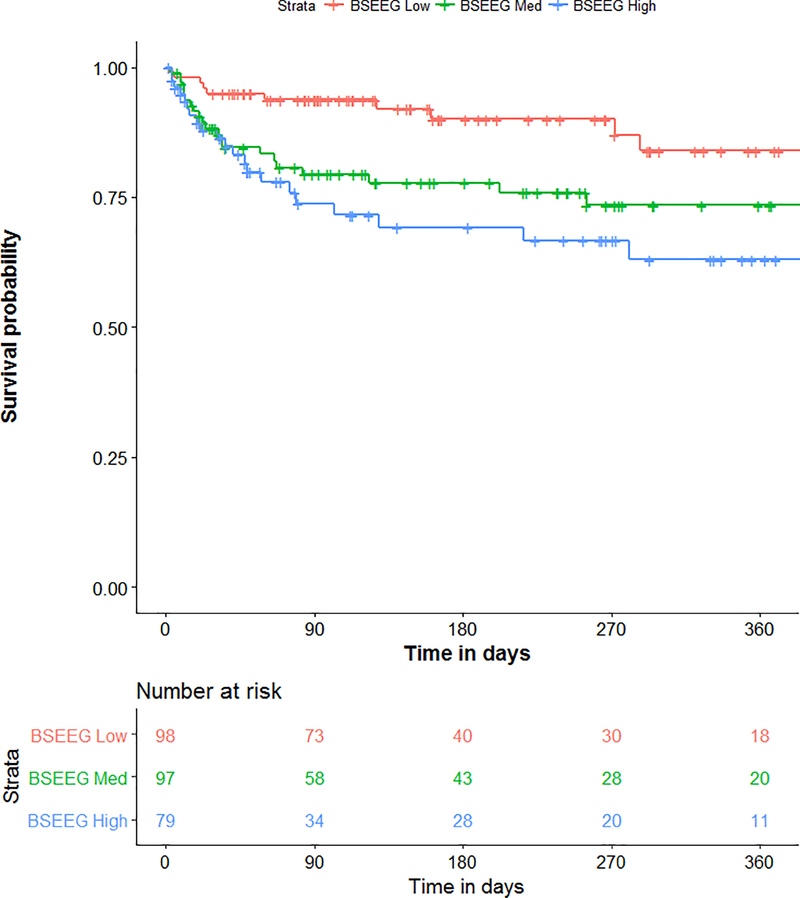
Results: A total of 274 patients had BSEEG score data available for analysis. Delirium and BSEEG score had a significant association (P < .001). Higher BSEEG scores were significantly correlated with length of stay (P < .001 unadjusted, P = .001 adjusted for age, sex, and Charlson Comorbidity Index [CCI] score) as well as with discharge not to home (P < .01). Hazard ratio for survival controlling for age, sex, CCI score, and delirium status was 1.35 (95% CI,1.04 to 1.76; P = .025).
Conclusions: In BSEEG, an efficient and reliable device that provides an objective measurement of delirium status was developed. The BSEEG score is significantly associated with pertinent clinical outcomes of mortality, hospital length of stay, and discharge disposition. The BSEEG score better predicts mortality than does clinical delirium status. This study identified a previously unrecognized subpopulation of patients without clinical features of delirium who are at increased mortality risk.
© Copyright 2019 Physicians Postgraduate Press, Inc.
Figures

References
-
- Inouye SK (2006). Delirium in older persons. N Engl J Med, 354(11), 1157–65. PMID: 16540616. - PubMed
-
- Ely EW, Stephens RK, Jackson JC, Thomason JW, Truman B, Gordon S, Dittus RS, Bernard GR (2004). Current opinions regarding the importance, diagnosis, and management of delirium in the intensive care unit: a survey of 912 healthcare professionals. Crit Care Med, 32(1), 106–12. PMID: 14707567. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
