

No radiographic wrist damage after treatment to target in recent-onset juvenile idiopathic arthritis
- PMID: 31484539
- PMCID: PMC6727344
- DOI: 10.1186/s12969-019-0362-1
No radiographic wrist damage after treatment to target in recent-onset juvenile idiopathic arthritis
Abstract
Background: To evaluate radiographic progression of patients with new-onset juvenile idiopathic arthritis (JIA) in response to an early, tightly-controlled, treatment-to-target.
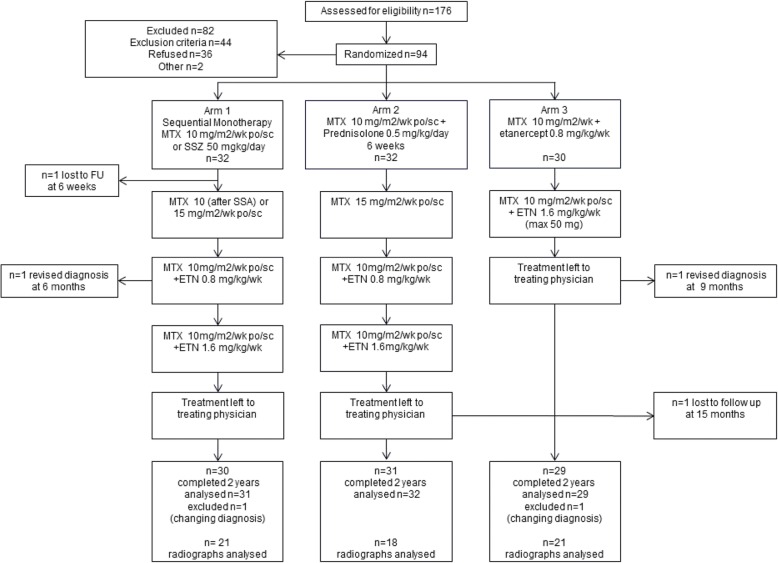
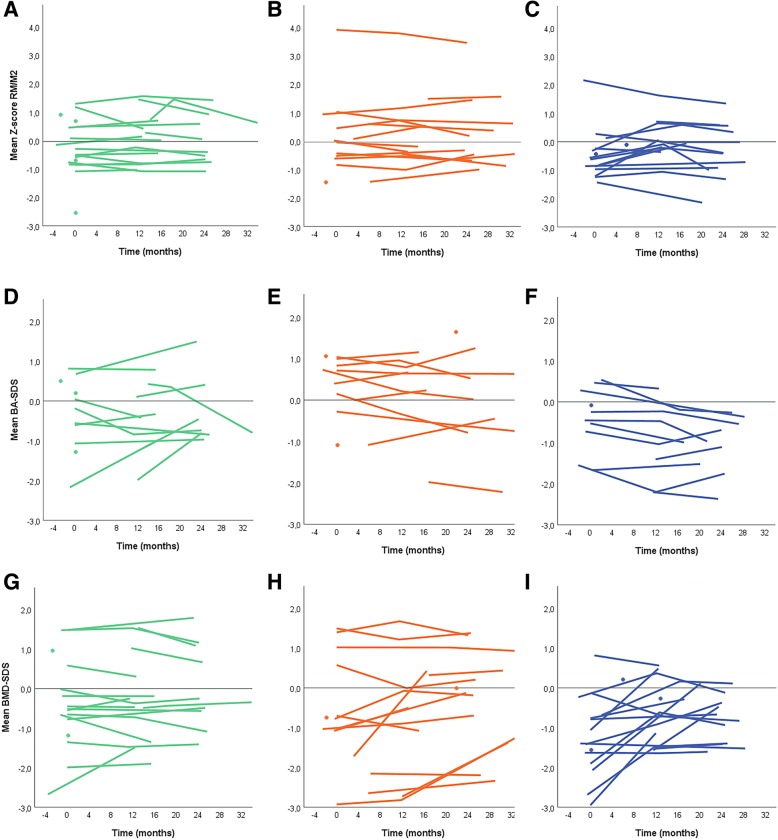
Methods: Patients with JIA participating in the BeSt-for-Kids-study, randomized to 3 treatment strategy arms, were eligible if at least 1 conventional wrist-radiograph was available. Bone damage as reflected by carpal length was assessed using the Poznanski-score. The BoneXpert-method was used to determine the Bone Age (BA, > 5 years) and bone mineral density (BMD) of the wrist. These scores were evaluated over time and compared between the treatment arms and mean JADAS10-score using linear mixed models corrected for age and symptom duration.
Results: In 60 patients, 252 radiographs were analysed. Baseline age and symptom duration were different between the arms. No difference in comparison to the healthy reference population was found at baseline for the Poznanski-score (IQR varying from - 0,82; 0.68), nor for BA (varying from - 0.88 to 0.74). Baseline BMD was statistically significantly lower in arm 3 (initial treatment with etanercept and methotrexate) (- 1.48; - 0.68) compared to arm 1 (- 0.84; - 0.04) and arm 2 (- 0.93; 0.15). After treatment to target inactive disease, the Poznanski-scores and the BA remained clinically unchanged, while the BMD in arm 3 improved (p < 0.05 vs arm 1).
Conclusions: Recent-onset JIA patients, treated-to-target aimed at inactive disease, showed no signs of radiographic wrist damage (Poznanski-score, BA or BMD) either at baseline or at follow-up, irrespective of treatment arm. A lower BMD at baseline in arm 3, initially treated with methotrexate and etanercept, improved significantly after treatment.
Trial registration: NTR, NL1504 (NTR1574). Registered 01-06-2009.
Keywords: Conventional radiography; Juvenile idiopathic arthritis; Radiographic outcome; Treatment to target.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Increasing the etanercept dose in a treat-to-target approach in juvenile idiopathic arthritis: does it help to reach the target? A post-hoc analysis of the BeSt for Kids randomised clinical trial.Pediatr Rheumatol Online J. 2024 May 10;22(1):53. doi: 10.1186/s12969-024-00989-x. Pediatr Rheumatol Online J. 2024. PMID: 38730442 Free PMC article. Clinical Trial.
-
Treat to target (drug-free) inactive disease in DMARD-naive juvenile idiopathic arthritis: 24-month clinical outcomes of a three-armed randomised trial.Ann Rheum Dis. 2019 Jan;78(1):51-59. doi: 10.1136/annrheumdis-2018-213902. Epub 2018 Oct 11. Ann Rheum Dis. 2019. PMID: 30309970 Clinical Trial.
-
Tocilizumab may slow radiographic progression in patients with systemic or polyarticular-course juvenile idiopathic arthritis: post hoc radiographic analysis from two randomized controlled trials.Arthritis Res Ther. 2020 Sep 10;22(1):211. doi: 10.1186/s13075-020-02303-y. Arthritis Res Ther. 2020. PMID: 32912276 Free PMC article.
-
A comparison of three treatment strategies in recent onset non-systemic Juvenile Idiopathic Arthritis: initial 3-months results of the BeSt for Kids-study.Pediatr Rheumatol Online J. 2017 Feb 6;15(1):11. doi: 10.1186/s12969-017-0138-4. Pediatr Rheumatol Online J. 2017. PMID: 28166785 Free PMC article. Clinical Trial.
-
Etanercept: an updated review of its use in rheumatoid arthritis, psoriatic arthritis and juvenile rheumatoid arthritis.Drugs. 2002;62(17):2493-537. doi: 10.2165/00003495-200262170-00013. Drugs. 2002. PMID: 12421111 Review.
Cited by
-
Patterns of clinical joint inflammation in juvenile idiopathic arthritis.RMD Open. 2023 Mar;9(1):e002941. doi: 10.1136/rmdopen-2022-002941. RMD Open. 2023. PMID: 36927851 Free PMC article.
-
Tumor necrosis factor (TNF) inhibitors for juvenile idiopathic arthritis.Cochrane Database Syst Rev. 2025 Feb 20;2(2):CD013715. doi: 10.1002/14651858.CD013715.pub2. Cochrane Database Syst Rev. 2025. PMID: 39976227
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. - PubMed
-
- Ravelli A, Ioseliani M, Norambuena X, Sato J, Pistorio A, Rossi F, et al. Adapted versions of the sharp/van der Heijde score are reliable and valid for assessment of radiographic progression in juvenile idiopathic arthritis. Arthritis Rheum. 2007;56(9):3087–3095. doi: 10.1002/art.22835. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
