

Laparoscopic liver resection for non-colorectal non-neuroendocrine metastases: perioperative and oncologic outcomes
- PMID: 31484583
- PMCID: PMC6727573
- DOI: 10.1186/s12957-019-1700-y
Laparoscopic liver resection for non-colorectal non-neuroendocrine metastases: perioperative and oncologic outcomes
Abstract
Background: Liver resection is a treatment of choice for colorectal and neuroendocrine liver metastases, and laparoscopy is an accepted approach for surgical treatment of these patients. The role of liver resection for patients with non-colorectal non-neuroendocrine liver metastases (NCNNLM), however, is still disputable. Outcomes of laparoscopic liver resection for this group of patients have not been analyzed.
Material and methods: In this retrospective study, patients who underwent laparoscopic liver resection for NCNNLM at Oslo University Hospital between April 2000 and January 2018 were analyzed. Perioperative and oncologic data of these patients were examined. Postoperative morbidity was classified using the Accordion classification. Kaplan-Meier method was used for survival analysis. Median follow-up was 26 (IQR, 12-41) months.
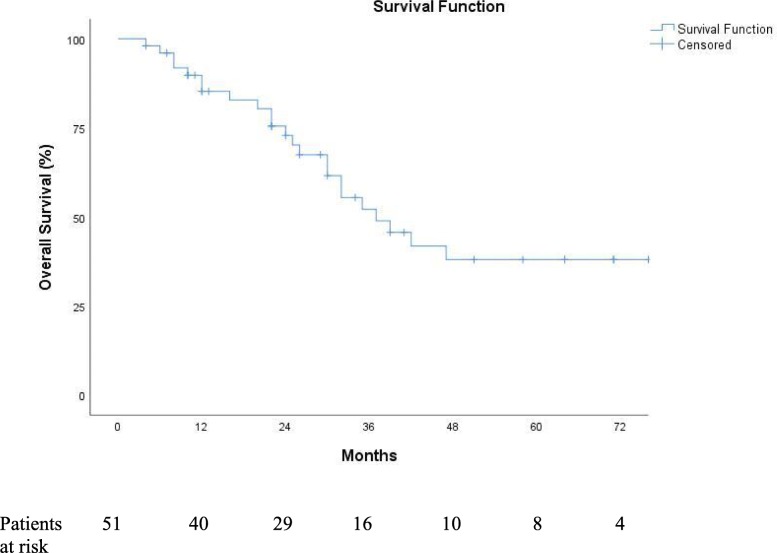
Results: Fifty-one patients were identified from a prospectively collected database. The histology of primary tumors was classified as adenocarcinoma (n = 16), sarcoma (n = 4), squamous cell carcinoma (n = 4), melanoma (n = 16), gastrointestinal stromal tumor (n = 9), and adrenocortical carcinoma (n = 2). The median operative time was 147 (IQR, 95-225) min, while the median blood loss was 200 (IQR, 50-500) ml. Nine (18%) patients experienced postoperative complications. There was no 90-day mortality in this study. Thirty-five (68%) patients developed disease recurrence or progression. Seven (14%) patients underwent repeat surgical procedure for recurrent liver metastases. One-, three-, and five-year overall survival rates were 85%, 52%, and 38%, respectively. The median overall survival was 37 (95%CI, 25 to 49) months.
Conclusion: Laparoscopic liver resection for NCNNLM results in good outcomes and should be considered in patients selected for surgical treatment.
Keywords: Laparoscopic liver surgery; Non-colorectal; Non-neuroendocrine liver metastases; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14(12):1208–1215. doi: 10.1016/S1470-2045(13)70447-9. - DOI - PubMed
-
- Pavel M, O'Toole D, Costa F, Capdevila J, Gross D, Kianmanesh R, et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology. 2016;103(2):172–185. doi: 10.1159/000443167. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
