

Mortality and respiratory support in X-linked myotubular myopathy: a RECENSUS retrospective analysis
- PMID: 31484632
- PMCID: PMC7054136
- DOI: 10.1136/archdischild-2019-317910
Mortality and respiratory support in X-linked myotubular myopathy: a RECENSUS retrospective analysis
Abstract
Purpose: Individuals with X-linked myotubular myopathy (XLMTM) who survive infancy require extensive supportive care, including ventilator assistance, wheelchairs and feeding tubes. Half die before 18 months of age. We explored respiratory support and associated mortality risk in RECENSUS, particularly among patients ≤5 years old who received respiratory support at birth; this subgroup closely matches patients in the ASPIRO trial of gene therapy for XLMTM.
Design: RECENSUS is an international, retrospective study of patients with XLMTM. Descriptive and time-to-event analyses examined survival on the basis of age, respiratory support, tracheostomy use, predicted mutational effects and life-sustaining care.
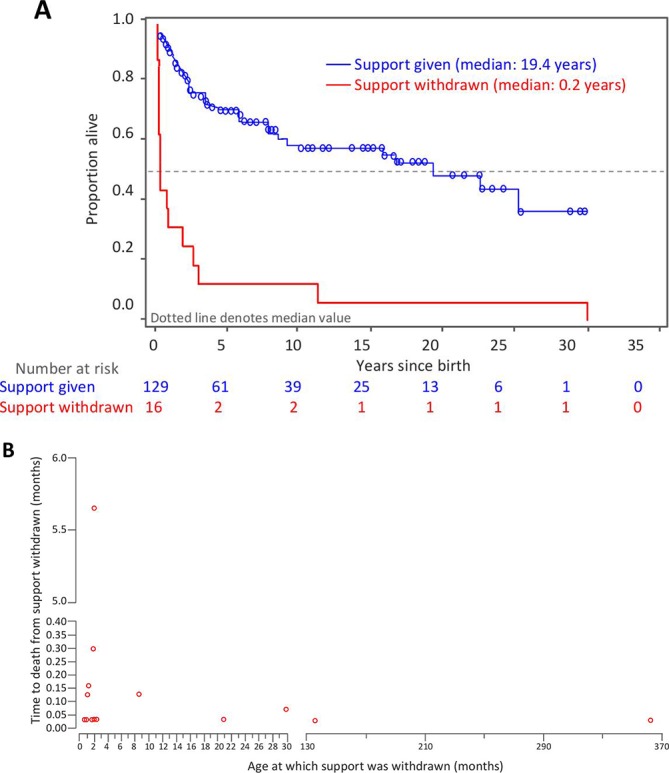
Results: Outcomes for 145 patients were evaluated. Among 126 patients with respiratory support at birth, mortality was 47% overall and 59% among those ≤5 years old. Median survival time was shorter for patients ≤5 years old than for those >5 years old (2.2 years (IQR 0.7-5.6) vs 30.2 years (IQR 19.4-30.2)). The most common cause of death was respiratory failure (66.7%). Median survival time was longer for patients with a tracheostomy than for those without (22.8 years (IQR 8.7-30.2) vs 1.8 years (IQR 0.2-not estimable)). The proportion of patients living without a tracheostomy was 50% at age 6 months and 28% at age 2 years. Median survival time was longer with provision of life-sustaining care than without (19.4 years (IQR 3.1-not estimable) vs 0.2 years (IQR 0.1-2.1)).
Conclusions: High mortality, principally due to respiratory failure, among patients with XLMTM ≤5 years old despite respiratory support underscores the need for early diagnosis, informed decision-making and disease-modifying therapies.
Trial registration number: NCT02231697.
Keywords: X-linked myotubular myopathy; centronuclear myopathy; congenital myopathy; mortality; respiratory support; retrospective chart review; tracheostomy.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RJG, IH, MLY, NLK and SWY report no conflicts of interest with respect to this study. RJG is an unpaid member of Audentes Therapeutics Board of Scientific and Clinical Advisors. RA is a volunteer for Cure CMD and has no financial interest in Audentes or related to this study. LBL received financial compensation for medical writing, and TH is a consultant to Audentes Therapeutics. ESJ, MN, SR and SP are employees and shareholders of Audentes Therapeutics. AHB is a member of the Audentes Therapeutics Board of Scientific and Clinical Advisors and has received support from a sponsored research agreement with Audentes Therapeutics to cover running costs for this study.
Figures

References
-
- Dowling JJ, Lawlor MW, Das S. X-Linked Myotubular Myopathy : Adam MP, Ardinger HH, Pagon RA, GeneReviews((R))1993-2019. Seattle (WA), 2002.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical