

Macrolide-Resistant Mycoplasma pneumoniae in the United States as Determined from a National Surveillance Program
- PMID: 31484701
- PMCID: PMC6813023
- DOI: 10.1128/JCM.00968-19
Macrolide-Resistant Mycoplasma pneumoniae in the United States as Determined from a National Surveillance Program
Abstract
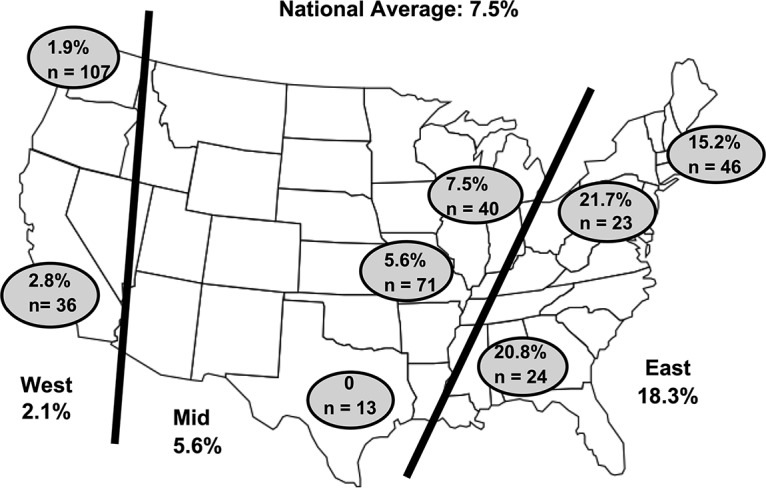
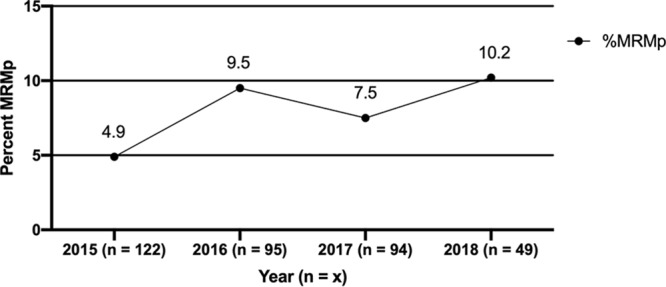
There are sparse data to indicate the extent that macrolide-resistant Mycoplasma pneumoniae (MRMp) occurs in the United States or its clinical significance. Between 2015 and 2018, hospitals in 8 states collected and stored respiratory specimens that tested positive for M. pneumoniae and sent them to the University of Alabama at Birmingham, where real-time PCR was performed for detection of 23S rRNA mutations known to confer macrolide resistance. MRMp was detected in 27 of 360 specimens (7.5%). MRMp prevalence was significantly higher in the South and East (18.3%) than in the West (2.1%). A2063G was the predominant 23S rRNA mutation detected. MICs for macrolide-susceptible M. pneumoniae (MSMp) were ≤0.008 μg/ml, whereas MICs for MRMp were 16 to 32 μg/ml. Patients with MRMp infection were more likely to have a history of immunodeficiency or malignancy. Otherwise, there were no other significant differences in the clinical features between patients infected with MRMp and those infected with MSMp, nor were there any differences in radiographic findings, hospitalization rates, viral coinfections, the mean duration of antimicrobial treatment, or clinical outcomes. There was no significant change in MRMp incidence over time or according to age, sex, race/ethnicity, or status as an inpatient or an outpatient. Patients with MRMp were more likely to have received a macrolide prior to presentation, and their treatment was more likely to have been changed to a fluoroquinolone after presentation. This is the first national surveillance program for M. pneumoniae in the United States. Additional surveillance is needed to assess the clinical significance of MRMp and to monitor changes in MRMp prevalence.
Keywords: Mycoplasma pneumoniae; antibiotic resistance; macrolide; surveillance.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, Stockmann C, Anderson EJ, Grijalva CG, Self WH, Zhu Y, Patel A, Hymas W, Chappell JD, Kaufman RA, Kan JH, Dansie D, Lenny N, Hillyard DR, Haynes LM, Levine M, Lindstrom S, Winchell JM, Katz JM, Erdman D, Schneider E, Hicks LA, Wunderink RG, Edwards KM, Pavia AT, McCullers JA, Finelli L, CDC EPIC Study Team . 2015. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med 372:835–845. doi: 10.1056/NEJMoa1405870. - DOI - PMC - PubMed
-
- Jain S, Self WH, Wunderink RG, Fakhran S, Balk R, Bramley AM, Reed C, Grijalva CG, Anderson EJ, Courtney DM, Chappell JD, Qi C, Hart EM, Carroll F, Trabue C, Donnelly HK, Williams DJ, Zhu Y, Arnold SR, Ampofo K, Waterer GW, Levine M, Lindstrom S, Winchell JM, Katz JM, Erdman D, Schneider E, Hicks LA, McCullers JA, Pavia AT, Edwards KM, Finelli L, CDC EPIC Study Team . 2015. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med 373:415–427. doi: 10.1056/NEJMoa1500245. - DOI - PMC - PubMed
-
- Winchell JM. 2013. Mycoplasma pneumoniae—a national public health perspective. Curr Pediatr Rev 9:324–333. doi: 10.2174/15733963113099990009. - DOI
-
- Gadsby NJ, Reynolds AJ, McMenamin J, Gunson RN, McDonagh S, Molyneaux PJ, Yirrell DL, Templeton KE. 2012. Increased reports of Mycoplasma pneumoniae from laboratories in Scotland in 2010 and 2011—impact of the epidemic in infants. Euro Surveill 17(10):pii=20110 10.2807/ese.17.10.20110-en. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
