

Clinical Evaluation of Melorheostosis in the Context of a Natural History Clinical Study
- PMID: 31485554
- PMCID: PMC6715778
- DOI: 10.1002/jbm4.10214
Clinical Evaluation of Melorheostosis in the Context of a Natural History Clinical Study
Abstract
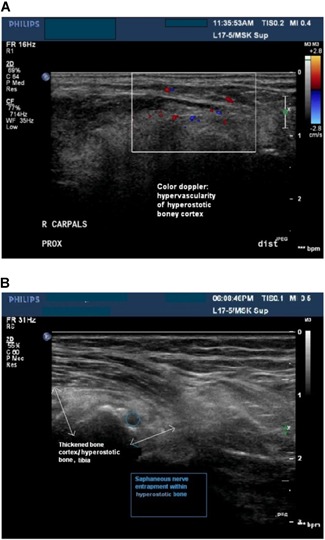
Melorheostosis is a rare dysostosis involving cortical bone overgrowth that affects the appendicular skeleton. Patients present with pain, deformities, contractures, range of motion limitation(s), and limb swelling. It has been described in children as well as adults. We recently identified somatic mosaicism for gain-of-function mutations in MAP2K1 in patients with melorheostosis. Despite these advances in genetic understanding, there are no effective therapies or clinical guidelines to help clinicians and patients in disease management. In a study to better characterize the clinical and genetic aspects of the disease, we recruited 30 adults with a radiographic appearance of melorheostosis and corresponding increased uptake on 18F-NaF positron emission tomography (PET)/CT. Patients underwent physical exam, imaging studies, and laboratory assessment. All patients underwent nerve conduction studies and ultrasound imaging of the nerve in the anatomic distribution of melorheostosis. We found sensory deficits in approximately 77% of patients, with evidence of focal nerve entrapment in five patients. All patients reported pain; 53% of patients had changes in skin overlying the affected bone. No significant laboratory abnormalities were noted. Our findings suggest that patients with melorheostosis may benefit from a multidisciplinary team of dermatologists, neurologists, orthopedic surgeons, pain and palliative care specialists, and physical medicine and rehabilitation specialists. Future studies focused on disease management are needed. © 2019 The Authors. JBMR Plus Published by Wiley Periodicals, Inc. on behalf of American Society for Bone and Mineral Research.
Keywords: CANDLE‐WAX DISEASE; LERI'S DISEASE; MAP2K1; SCLEROTIC; SOMATIC MOSAIC.
Figures



Similar articles
-
Melorheostosis (Leri's Disease): A Review.Cureus. 2024 Jun 8;16(6):e61950. doi: 10.7759/cureus.61950. eCollection 2024 Jun. Cureus. 2024. PMID: 38978887 Free PMC article. Review.
-
Cross-Sectional Imaging Useful in Melorheostosis.JBMR Plus. 2021 Feb 18;5(4):e10472. doi: 10.1002/jbm4.10472. eCollection 2021 Apr. JBMR Plus. 2021. PMID: 33869990 Free PMC article.
-
Distinct Clinical and Pathological Features of Melorheostosis Associated With Somatic MAP2K1 Mutations.J Bone Miner Res. 2019 Jan;34(1):145-156. doi: 10.1002/jbmr.3577. Epub 2018 Sep 14. J Bone Miner Res. 2019. PMID: 30138550 Free PMC article. Clinical Trial.
-
Melorheostosis: a Rare Sclerosing Bone Dysplasia.Curr Osteoporos Rep. 2017 Aug;15(4):335-342. doi: 10.1007/s11914-017-0375-y. Curr Osteoporos Rep. 2017. PMID: 28676968 Review.
-
Melorheostosis and Osteopoikilosis: A Review of Clinical Features and Pathogenesis.Calcif Tissue Int. 2019 May;104(5):530-543. doi: 10.1007/s00223-019-00543-y. Epub 2019 Apr 15. Calcif Tissue Int. 2019. PMID: 30989250 Review.
Cited by
-
Melorheostosis (Leri's Disease): A Review.Cureus. 2024 Jun 8;16(6):e61950. doi: 10.7759/cureus.61950. eCollection 2024 Jun. Cureus. 2024. PMID: 38978887 Free PMC article. Review.
-
Fibroblasts from Patients with Melorheostosis Promote Angiogenesis in Healthy Endothelial Cells through Secreted Factors.J Invest Dermatol. 2022 Sep;142(9):2406-2414.e5. doi: 10.1016/j.jid.2022.02.006. Epub 2022 Feb 19. J Invest Dermatol. 2022. PMID: 35189151 Free PMC article.
-
Unraveling melorheostosis: insights into clinical features, diagnosis, and treatment.JBMR Plus. 2024 Dec 11;9(2):ziae163. doi: 10.1093/jbmrpl/ziae163. eCollection 2025 Feb. JBMR Plus. 2024. PMID: 39776616 Free PMC article. Review.
-
Cross-Sectional Imaging Useful in Melorheostosis.JBMR Plus. 2021 Feb 18;5(4):e10472. doi: 10.1002/jbm4.10472. eCollection 2021 Apr. JBMR Plus. 2021. PMID: 33869990 Free PMC article.
-
Bone Material Properties in Bone Diseases Affecting Children.Curr Osteoporos Rep. 2023 Dec;21(6):787-805. doi: 10.1007/s11914-023-00822-6. Epub 2023 Oct 28. Curr Osteoporos Rep. 2023. PMID: 37897675 Review.
References
-
- Wynne‐Davies R, Gormley J. The prevalence of skeletal dysplasias. An estimate of their minimum frequency and the number of patients requiring orthopedic care. J Bone Joint Surg Br. 1985;67‐B(1):133–7. - PubMed
-
- Wordsworth P, Chan M. Melorheostosis and osteopoikilosis: a review of clinical features and pathogenesis. Calcif Tissue Int. 2019;104(5):530–43. - PubMed
-
- Hellemans J, Preobrazhenska O, Willaert A, et al. Loss‐of‐function mutations in LEMD3 result in osteopoikilosis, Buschke‐Ollendorff syndrome and melorheostosis. Nat Genet. 2004;36(11):1213–8. - PubMed
-
- Hellemans J, Debeer P, Wright M, et al. Germline LEMD3 mutations are rare in sporadic patients with isolated melorheostosis. Hum Mutat. 2006;27(3):290. - PubMed
-
- Mumm S, Wenkert D, Zhang X, McAlister WH, Mier RJ, Whyte MP. Deactivating germline mutations in LEMD3 cause osteopoikilosis and Buschke‐Ollendorff syndrome, but not sporadic melorheostosis. J Bone Miner Res. 2007;22(2):243–50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous