

The association between medication non-adherence and adverse health outcomes in ageing populations: A systematic review and meta-analysis
- PMID: 31486099
- PMCID: PMC6848955
- DOI: 10.1111/bcp.14075
The association between medication non-adherence and adverse health outcomes in ageing populations: A systematic review and meta-analysis
Abstract
Aims: The aim of this systematic review and meta-analysis was to synthesise the evidence relating to medication non-adherence and its association with health outcomes in people aged ≥50 years.
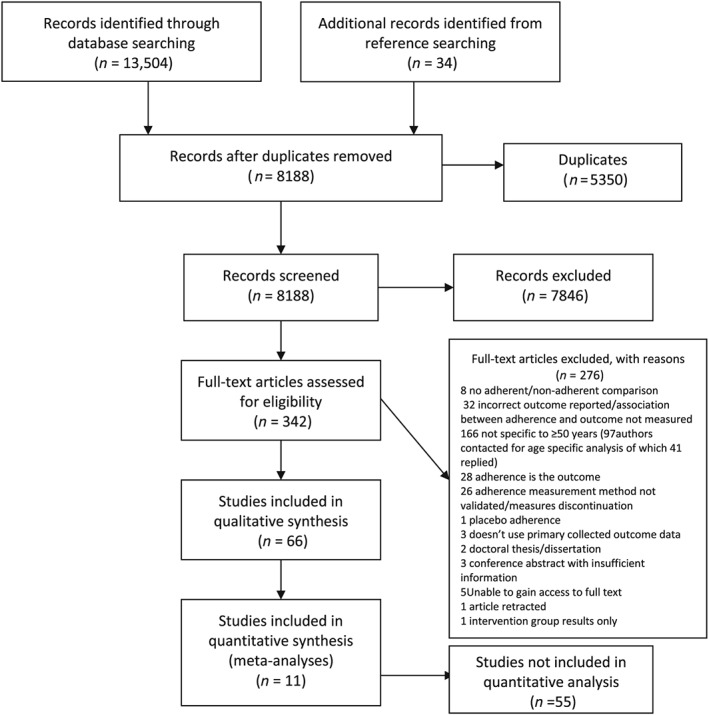
Methods: Seven databases were searched up to February 2019 for observational studies that measured medication (non-)adherence as a predictor of the following health outcomes in adults aged ≥50 years: healthcare utilisation (hospitalisation, emergency department visits, outpatient visits and general practitioner visits), mortality, adverse clinical events and quality of life. Screening and quality assessment using validated criteria were completed by 2 reviewers independently. Random effects models were used to generate pooled estimates of association using adjusted study results. The full methodological approach was published on PROSPERO (ID: CRD42017077264).
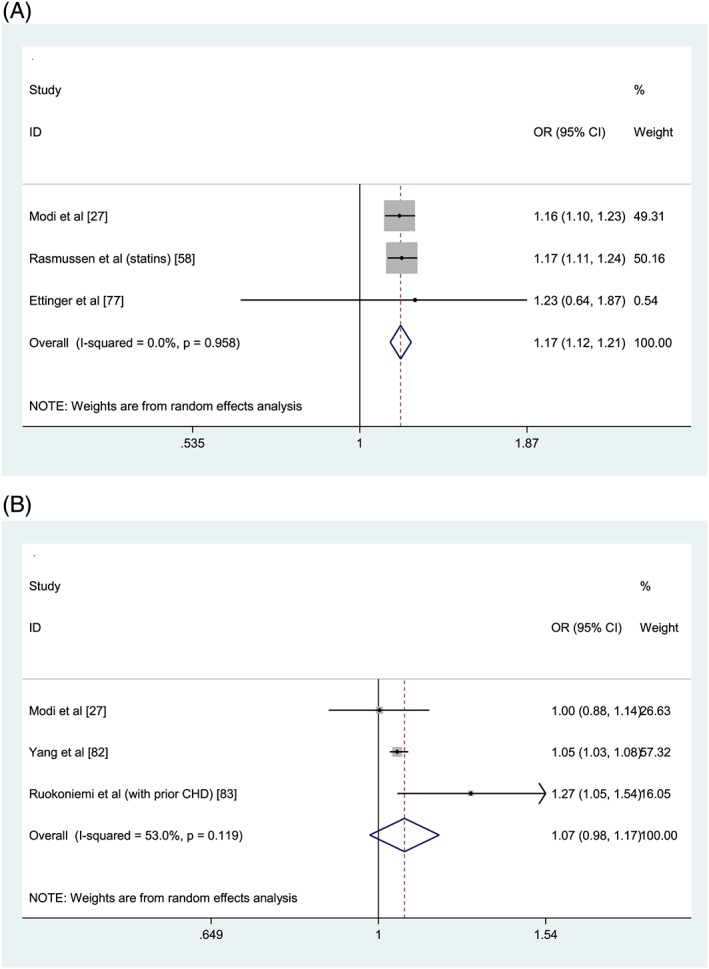
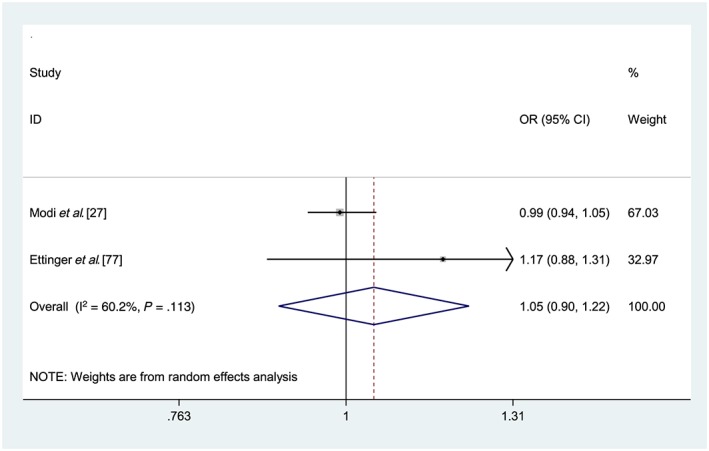
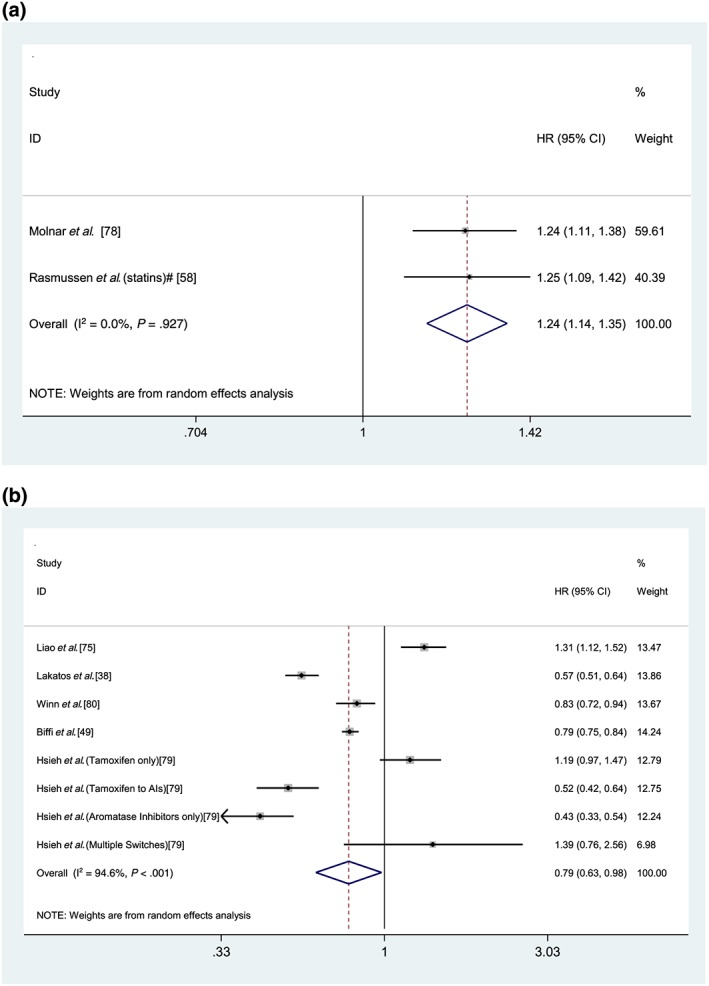
Results: Sixty-six studies were identified for qualitative synthesis, with 11 of these studies eligible for meta-analyses. A meta-analysis including 3 studies measuring medication non-adherence in adults aged ≥55 years showed a significant association with all-cause hospitalisation (adjusted odds ratio 1.17, 95% confidence interval [CI] 1.12, 1.21). A meta-analysis including 2 studies showed that medication non-adherence was not significantly associated with an emergency department visit (adjusted odds ratio 1.05, 95% CI 0.90, 1.22). Good adherence was associated with a 21% reduction in long-term mortality risk in comparison to medication non-adherence (adjusted hazard ratio 0.79, 95% CI 0.63, 0.98).
Conclusion: Medication non-adherence may be significantly associated with all-cause hospitalisation and mortality in older people. Medication adherence should be monitored and addressed in this cohort to minimise hospitalisation, improve clinical outcomes and reduce healthcare costs.
Keywords: ageing population; hospitalisation; medication adherence; mortality.
© 2019 The British Pharmacological Society.
Conflict of interest statement
There are no competing interests to declare.
Figures
References
-
- Hughes CM. Medication non‐adherence in the elderly. Drugs Aging. 2004;21(12):793‐811. - PubMed
-
- Vik SA, Hogan DB, Patten SB, Johnson JA, Romonko‐Slack L, Maxwell CJ. Medication nonadherence and subsequent risk of hospitalisation and mortality among older adults. Drugs Aging. 2006;23(4):345‐356. - PubMed
-
- Banning M. Older people and adherence with medication: a review of the literature. Int J Nurs Stud. 2008;45(10):1550‐1561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
