

Low-Value Proton Pump Inhibitor Prescriptions Among Older Adults at a Large Academic Health System
- PMID: 31486549
- PMCID: PMC6952216
- DOI: 10.1111/jgs.16117
Low-Value Proton Pump Inhibitor Prescriptions Among Older Adults at a Large Academic Health System
Abstract
Background: Older adults are particularly vulnerable to complications from proton pump inhibitor (PPI) drugs. We sought to characterize the prevalence of potentially low-value PPI prescriptions among older adults to inform a quality improvement (QI) intervention.
Methods: We created a cohort of patients, aged 65 years or older, receiving primary care at a large academic health system in 2018. We identified patients currently prescribed any PPI using the electronic health record (EHR) medication list (current defined as September 1, 2018). A geriatrician, a gastroenterologist, a QI expert, and two primary care physicians (PCPs) created multidisciplinary PPI appropriateness criteria based on evidenced-based guidelines. Supervised by a gastroenterologist and PCP, two internal medicine residents conducted manual chart reviews in a random sample of 399 patients prescribed PPIs. We considered prescriptions potentially low value if they lacked a guideline-based (1) short-term indication (gastroesophageal reflux disease [GERD]/peptic ulcer disease/Helicobacter pylori gastritis/dyspepsia) or (2) long-term (>8 weeks) indication (severe/refractory GERD/erosive esophagitis/Barrett esophagus/esophageal adenocarcinoma/esophageal stricture/high gastrointestinal bleeding risk/Zollinger-Ellison syndrome). We used the Wilson score method to calculate 95% confidence intervals (CIs) on low-value PPI prescription prevalence.
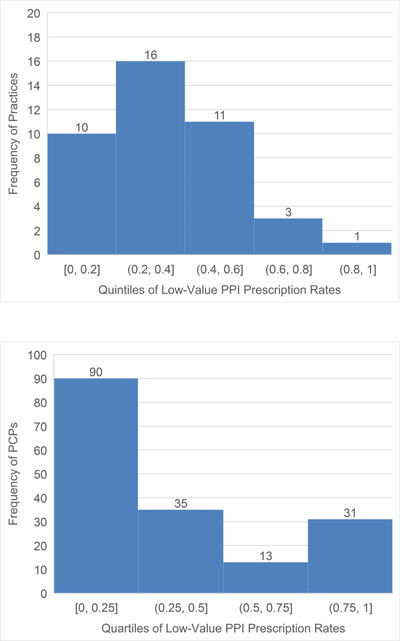
Results: Among 69 352 older adults, 8729 (12.6%) were prescribed a PPI. In the sample of 399 patients prescribed PPIs, 63.9% were female; their mean age was 76.2 years, and they were seen by 169 PCPs. Of the 399 prescriptions, 143 (35.8%; 95% CI = 31.3%-40.7%) were potentially low value-of which 82% began appropriately (eg, GERD) but then continued long term without a guideline-based indication. Among 169 PCPs, 32 (18.9%) contributed to 59.2% of potentially low-value prescriptions.
Conclusion: One in eight older adults were prescribed a PPI, and over one-third of prescriptions were potentially low-value. Most often, appropriate short-term prescriptions became potentially low value because they lacked long-term indications. With most potentially low-value prescribing concentrated among a small subset of PCPs, interventions targeting them and/or applying EHR-based automatic stopping rules may protect older adults from harm. J Am Geriatr Soc 67:2600-2604, 2019.
Keywords: deprescribing; geriatrics; high-value care; quality improvement; quality of care.
© 2019 The American Geriatrics Society.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- Kaiser Permanente Taking Action on Overuse Robert Wood Johnson Foundation Subaward/International
- K24 AG047899/AG/NIA NIH HHS/United States
- UCLA CTSI NIH/International
- 1U19HS024067-01/RAND Center of Excellence on Health System Performance/International
- KL2TR001882/National Center for Advanced Translational Science Institute (CTSI)/International
- KL2 TR001882/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- U19 HS024067/HS/AHRQ HHS/United States
- L1TR001881/National Center for Advanced Translational Science Institute (CTSI)/International
- National Institutes of Health (NIH)/International
- 1K24AG047899-01/AG/NIA NIH HHS/United States
