

Os Acromiale: Reviews and Current Perspectives
- PMID: 31486589
- PMCID: PMC6819188
- DOI: 10.1111/os.12518
Os Acromiale: Reviews and Current Perspectives
Abstract
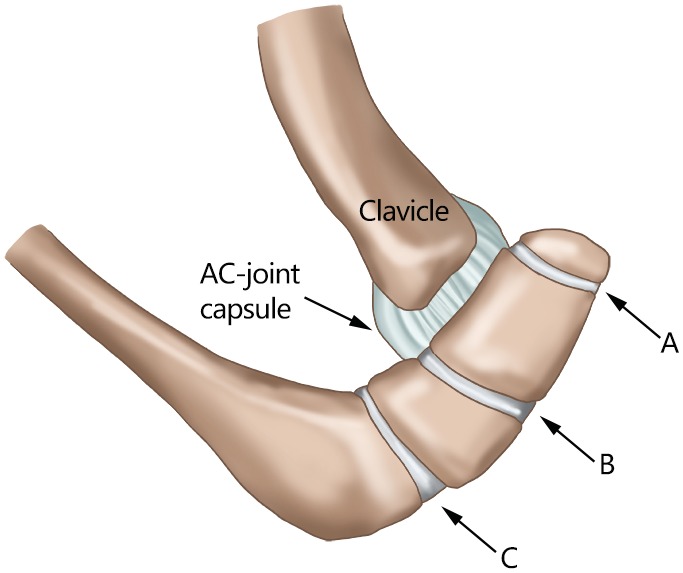
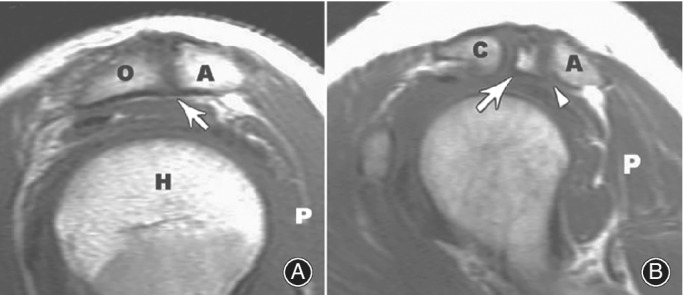
Os acromiale is a developmental defect which results from the lack of an osseous union between the ossification centers of the acromion, leading to the fibrocartilaginous tissue connection. The prevalence of os acromiale is 1% to 15%, and is quite common in the African American population. Os acromiale in adults is easily diagnosed by symptoms and X-ray, particularly on the axillary view; however, the differential diagnosis of adolescents may require MRI or SPECT-CT. Generally, nonoperative therapy for symptomatic os acromiale should be started, including physiotherapy, nonsteroidal anti-inflammatory drugs, and injections. Surgical treatment is indicated after failed conservative treatment. In symptomatic patients with fixable acromiale, the tension band technique should be used to make the anterior aspect of the acromion elevated from the humerus head. In patients with small fragments which are unsuitable for reattachment, excision might be the best therapeutic option and lead to good outcomes. Whether using internal fixation or resection, the arthroscopic technique results in a better outcome and fewer complications, especially in older patients or athletes with overhead movement, because of the high incidence of shoulder impingement or rotator cuff tears which can be treated concurrently.
Keywords: Arthroscopy; Os acromiale; Reverse shoulder arthroplasty; Rototar cuff tear; Shoulder impingement.
© 2019 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures






References
-
- Buss DD, Freehill MQ, Marra G. Typical and atypical shoulder impingement syndrome: diagnosis, treatment, and pitfalls. Instr Course Lect, 2009, 58: 447–457. - PubMed
-
- Maffulli N, Longo UG, Berton A, Loppini M, Denaro V. Biological factors in the pathogenesis of rotator cuff tears. Sports Med Arthrosc Rev, 2011, 19: 194–201. - PubMed
-
- Familiari F, Huri G, Gonzalez‐Zapata A, McFarland EG. Scapula fracture and os acromiale after reverse total shoulder arthroplasty. Orthopedics, 2014, 37: 434, 492–495. - PubMed
-
- Yammine K. The prevalence of os acromiale: a systematic review and meta‐analysis. Clin Anat, 2014, 27: 610–621. - PubMed
Publication types
MeSH terms
Grants and funding
- JCYJ20150403091443323/Science and Technology Program of Shenzhen, China
- A2017202/Medical Scientific Research Foundation of Guangdong Province, China
- 2017A030310616/Natural Science Foundation of Guangdong Province, China
- SZSM201612078/Sanming Project of Medicine in Shenzhen
- 201606007/Scientific Research Project of Health and Family Planning Commission of Shenzhen Municipality, China
LinkOut - more resources
Full Text Sources
