

The syringe potentiometer: a low-cost device for pneumotachograph calibration
- PMID: 31487222
- PMCID: PMC6850981
- DOI: 10.1152/japplphysiol.00150.2019
The syringe potentiometer: a low-cost device for pneumotachograph calibration
Abstract
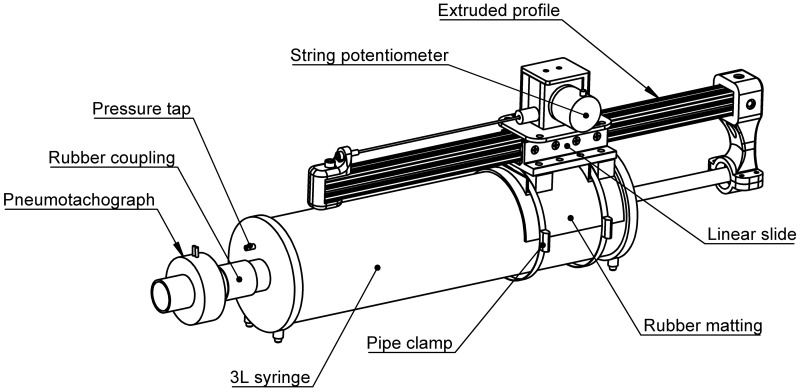
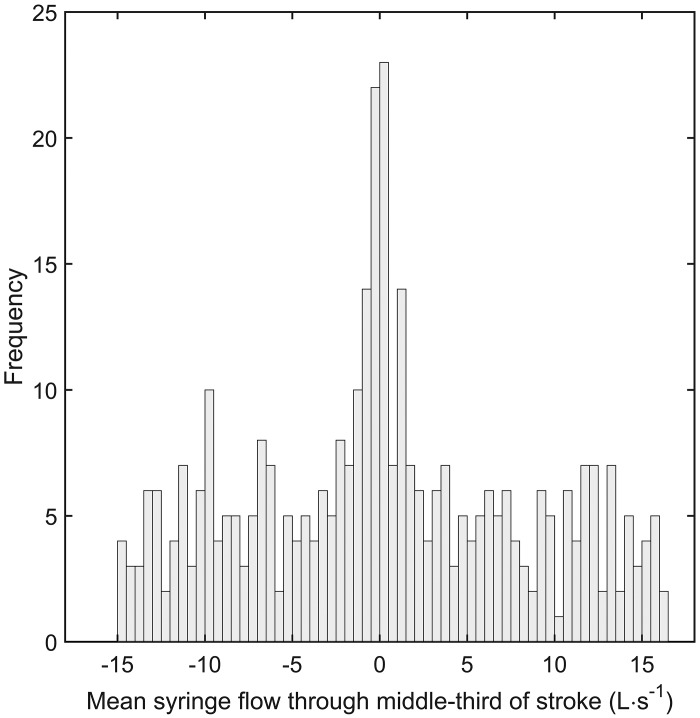
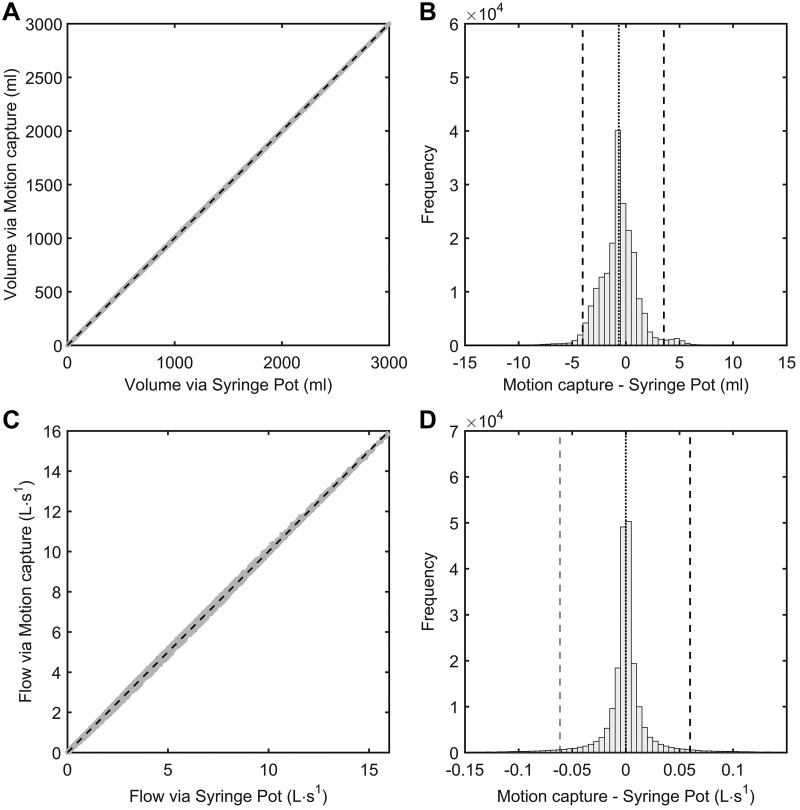
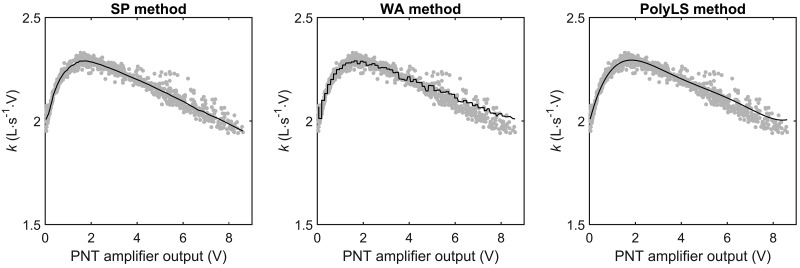
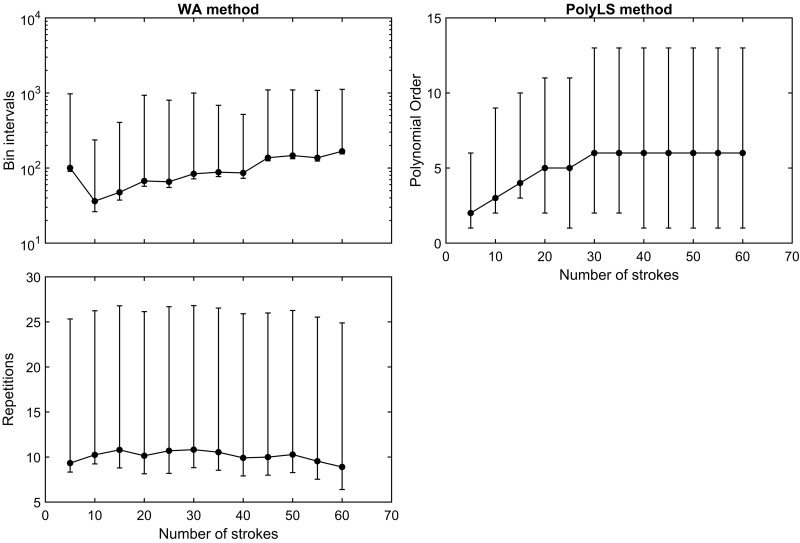
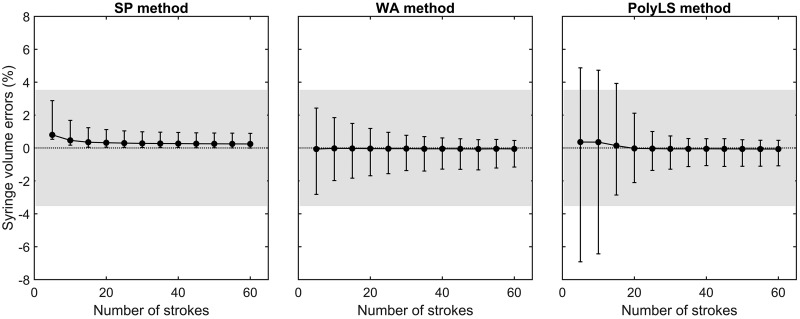
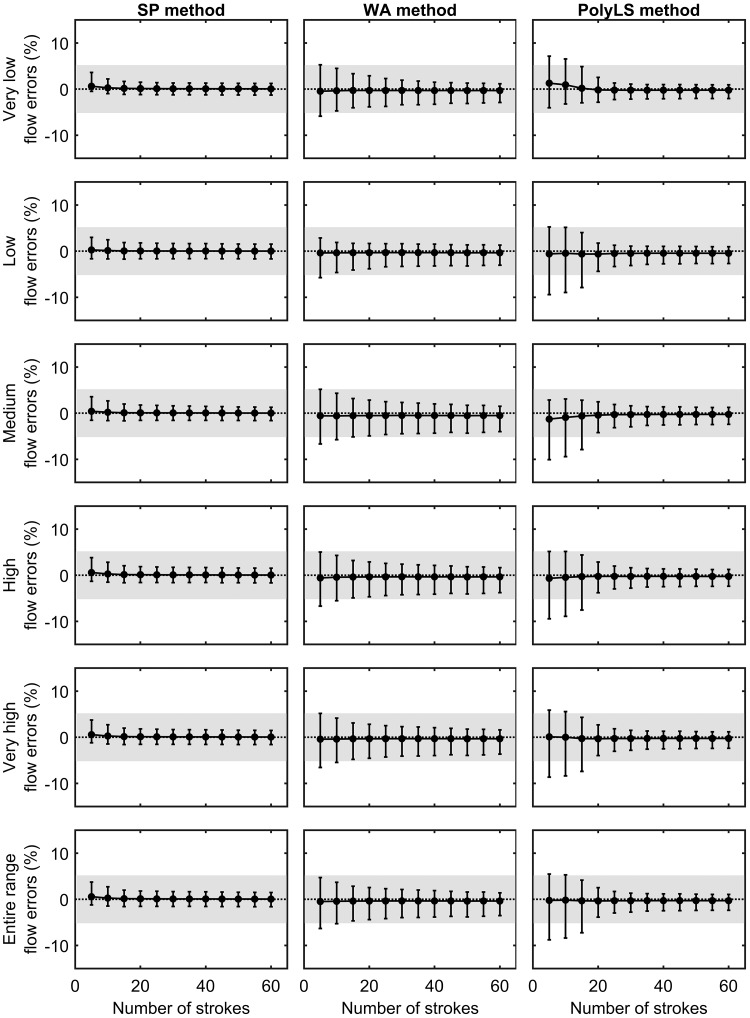
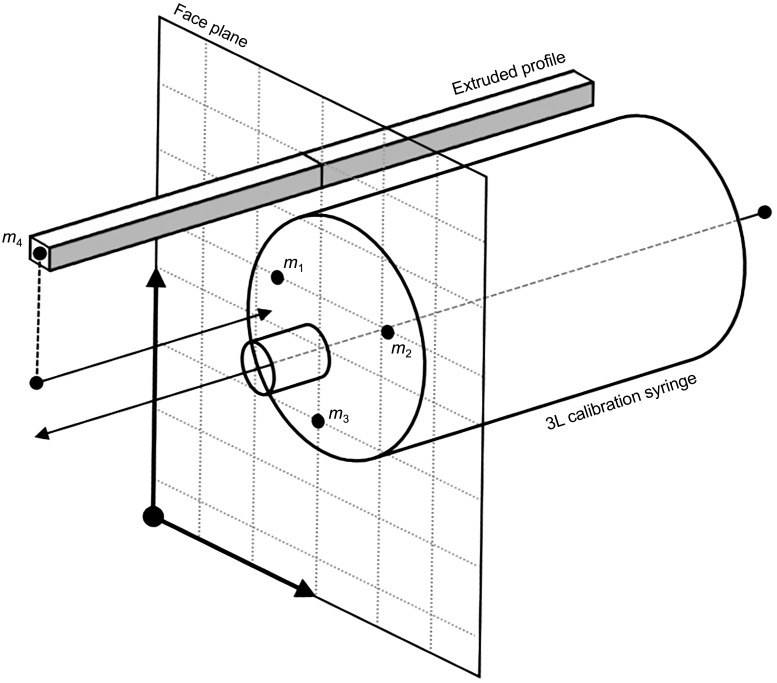
The purpose of this report was to 1) detail the construction of a low-cost device that provides a "reference" flow waveform for pneumotachograph (PNT) calibration, i.e., the "syringe potentiometer" (SP), and to compare the 2) accuracy and 3) practical performance of "calibration curves" obtained with the SP device to other more established methods of PNT calibration, i.e., the weighted averaging (WA) and polynomial least-squares (PolyLS) methods. Volume and flow waveforms obtained via the SP device were validated against a motion capture system and were deemed accurate surrogates of actual syringe volume and flows. The SP device was used to construct a calibration curve of a PNT by dividing the flow waveform of the SP by the analog output of the PNT amplifier. A total of 187 inspiratory and 187 expiratory strokes were collected. When the entire data set of expiratory strokes was used, the SP, WA, and PolyLS methods together demonstrated acceptable volume and flow errors as per American Thoracic Society/European Respiratory Society recommendations (less than ±3.5% and less than ±5.0% errors, respectively). The "practical" performance of each method was assessed with a nested subsampling procedure, whereby volume and flow errors were evaluated as the number of strokes was increased (in blocks of 5 strokes). To this end, the SP method demonstrated practical performance superior to that of the WA and PolyLS approaches, whereby acceptable volume and flow errors were achieved after only 5 calibration strokes; the WA and PolyLS methods required 15 and 20 strokes, respectively, to achieve the same level of volume and flow accuracy.NEW & NOTEWORTHY This report describes the construction and validation of a low-cost device for the purposes of pneumotachograph (PNT) calibration: the "syringe potentiometer" (SP). Calibration of a PNT with the SP device yielded acceptable volume and flow errors (<3.5% and 5%, respectively) across a wide range of flows (<0.5 to 15 L/s). The SP device offered superior "practical performance" over other established PNT calibration methods, whereby acceptable volume and flow errors were achieved after only five calibration strokes.
Keywords: calibration; pneumotachograph; potentiometer; respiratory airflow; syringe.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Breiman L, Friedman JH, Olshen RA, Stone CJ. Classification and Regression Trees. Belmont, CA: Wadsworth International Group, 1984.
-
- Friedman J. A Variable Span Smoother Laboratory for Computational Statistics (Technical Report 5). Stanford, CA: Stanford University, 1984.
-
- Hankinson JL, Reynolds JS, Das MK, Viola JO. Method to produce American Thoracic Society flow-time waveforms using a mechanical pump. Eur Respir J 10: 690–694, 1997. - PubMed
-
- Janabi-Sharifi F, Hayward V, Chen CS. Discrete-time adaptive windowing for velocity estimation. IEEE Trans Control Syst Technol 8: 1003–1009, 2000. doi:10.1109/87.880606. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources