Clinical Implication of Facial Nerve Decompression in Complete Bell's Palsy: A Systematic Review and Meta-Analysis
- PMID: 31487771
- PMCID: PMC6787481
- DOI: 10.21053/ceo.2019.00535
Clinical Implication of Facial Nerve Decompression in Complete Bell's Palsy: A Systematic Review and Meta-Analysis
Abstract
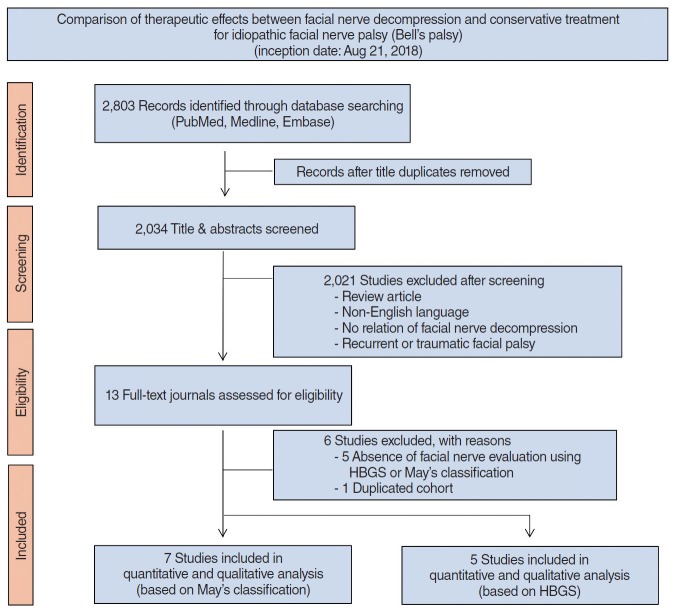
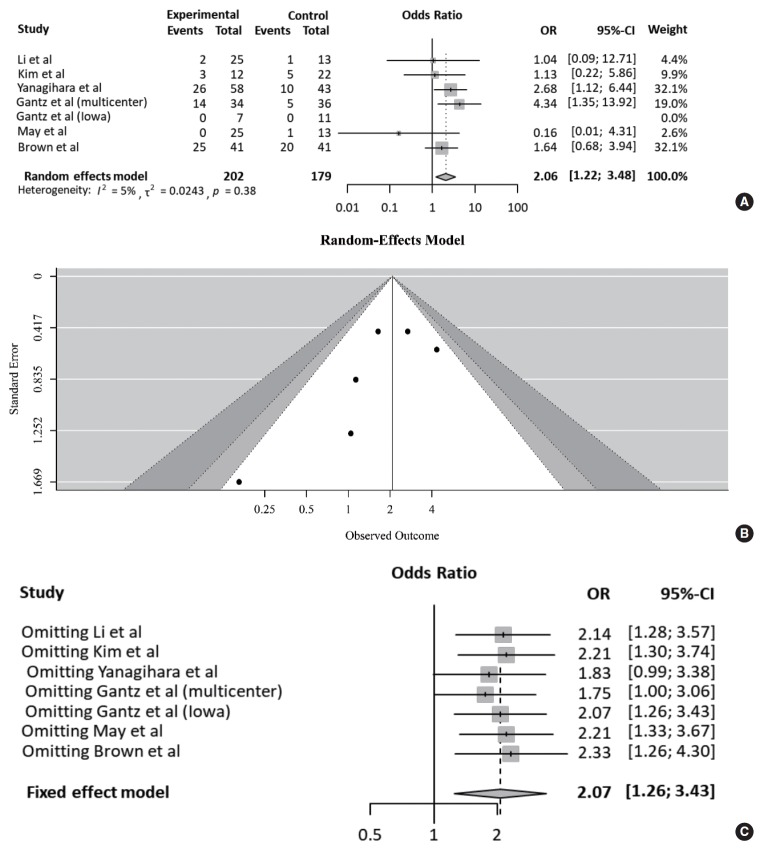
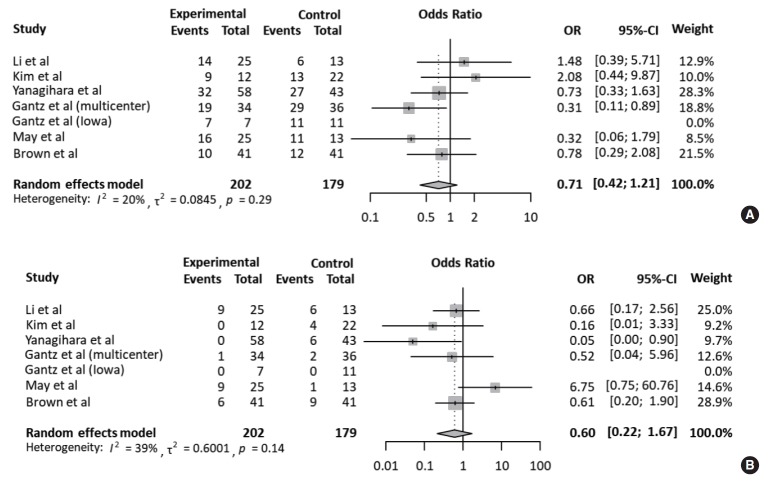
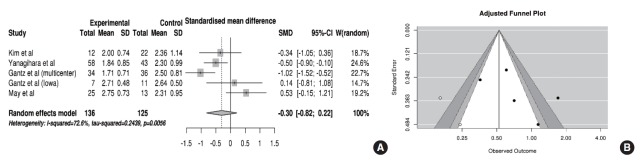
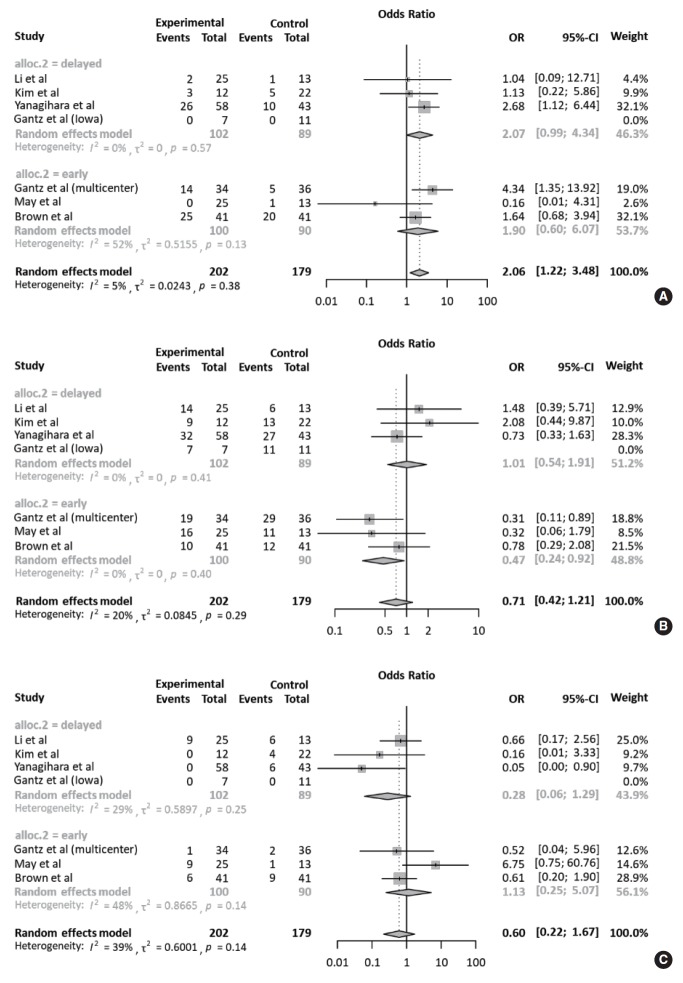
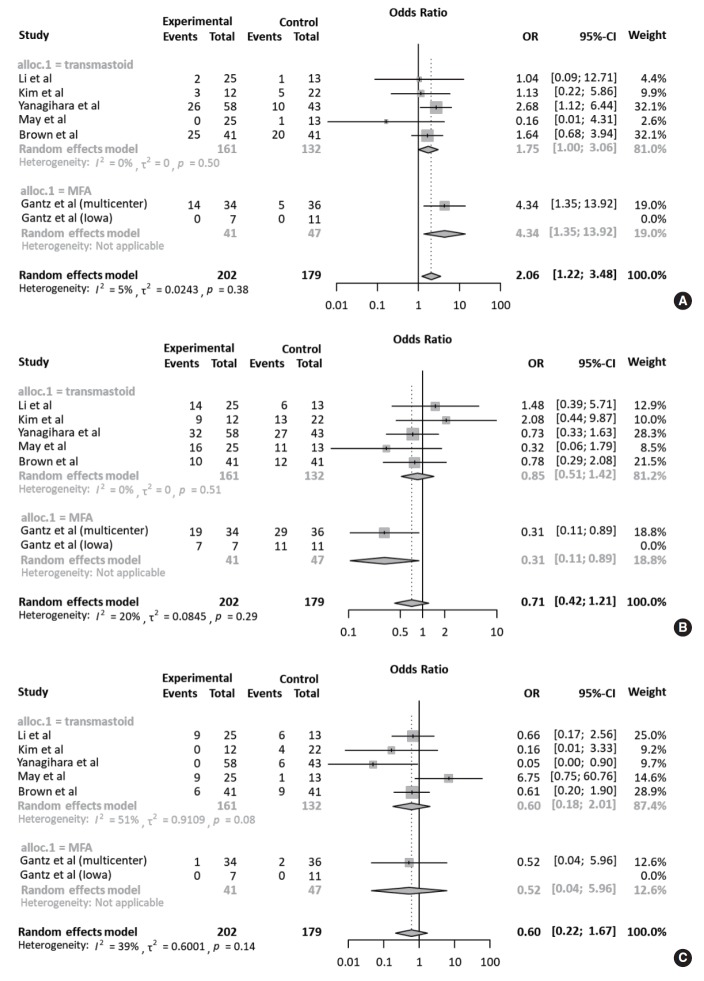
We compared the therapeutic efficacy of facial nerve decompression (FND) and conservative treatment in patients with Bell's palsy through a systematic review and meta-analysis. Primary database search was performed in PubMed, Medline, and Embase. After screening, 13 studies were assessed for their eligibility. Among them, seven studies employing either the House-Brackmann grading system (HBGS) or May's classification (modified HBGS) were selected for quantitative and qualitative analysis. Based on May's classification, the degree of recovery was classified into complete (HBGS I), fair (HBGS II-III), or failed (HBGS IV-VI) recovery. The outcomes were assessed between 6 and 12 months after surgery. The estimated pooled odds ratio (OR) and 95% confidence interval (CI) were calculated using random effects model. Cohorts were comprised of patients who underwent FND (n=202, 53.0%) and conservative treatments (n=179, 47.0%). In pooled analysis, the rate of complete recovery was significantly higher in the FND group than in the control group (OR, 2.06; 95% CI, 1.22 to 3.48; P=0.007) showing neither heterogeneity nor publication bias. Meanwhile, the rates of fair recovery (OR, 0.71; 95% CI, 0.42 to 1.21; P=0.208) and failed recovery (OR, 0.60; 95% CI, 0.22 to 1.67; P=0.327) in the FND group were similar to that in the control group. In subgroup analyses, there was no significant difference in the OR according to the operation timing and surgical approach. FND can be a possible treatment option for patients with complete Bell's palsy, especially for complete recovery, which provide insights on decision-making and outcome prediction. However, FND should be determined carefully given the risk of small study effects and possible complications.
Keywords: Bell Palsy; Facial Nerve Decompression; Meta-Analysis.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Sun DQ, Andresen NS, Gantz BJ. Surgical management of acute facial palsy. Otolaryngol Clin North Am. 2018 Dec;51(6):1077–92. - PubMed
-
- Peitersen E. Natural history of Bell’s palsy. Acta Otolaryngol Suppl. 1992;492:122–4. - PubMed
-
- Andresen NS, Sun DQ, Hansen MR. Facial nerve decompression. Curr Opin Otolaryngol Head Neck Surg. 2018 Oct;26(5):280–5. - PubMed
-
- Mantsopoulos K, Psillas G, Psychogios G, Brase C, Iro H, Constantinidis J. Predicting the long-term outcome after idiopathic facial nerve paralysis. Otol Neurotol. 2011 Jul;32(5):848–51. - PubMed