

Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: a cluster randomised controlled trial
- PMID: 31488140
- PMCID: PMC6729097
- DOI: 10.1186/s12966-019-0840-3
Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: a cluster randomised controlled trial
Abstract
Background: Most physical activity interventions in children focus on the school setting; however, children typically engage in more sedentary activities and spend more time eating when at home. The primary aim of this cluster randomised controlled trial was to investigate the effects of a compulsory, health-related homework programme on physical activity, dietary patterns, and body size in primary school-aged children.
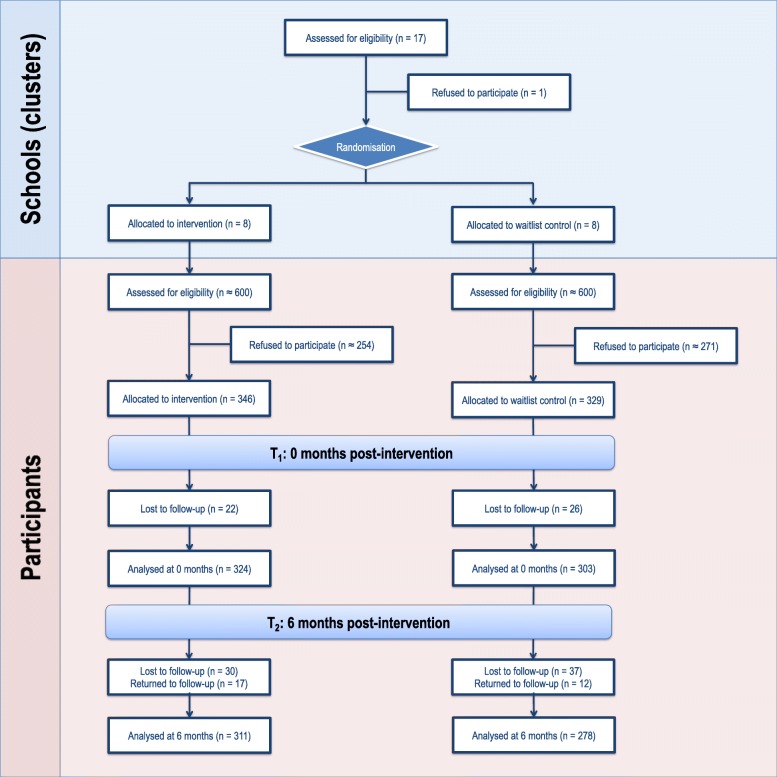
Methods: A total of 675 children aged 7-10 years from 16 New Zealand primary schools participated in the Healthy Homework study. Schools were randomised into intervention and control groups (1:1 allocation). Intervention schools implemented an 8-week applied homework and in-class teaching module designed to increase physical activity and improve dietary patterns. Physical activity was the primary outcome measure, and was assessed using two sealed pedometers that monitored school- and home-based activity separately. Secondary outcome measures included screen-based sedentary time and selected dietary patterns assessed via parental proxy questionnaire. In addition, height, weight, and waist circumference were measured to obtain body mass index (BMI) and waist-to-height ratio (WHtR). All measurements were taken at baseline (T0), immediately post-intervention (T1), and 6-months post-intervention (T2). Changes in outcome measures over time were estimated using generalised linear mixed models (GLMMs) that adjusted for fixed (group, age, sex, group x time) and random (subjects nested within schools) effects. Intervention effects were also quantified using GLMMs adjusted for baseline values.
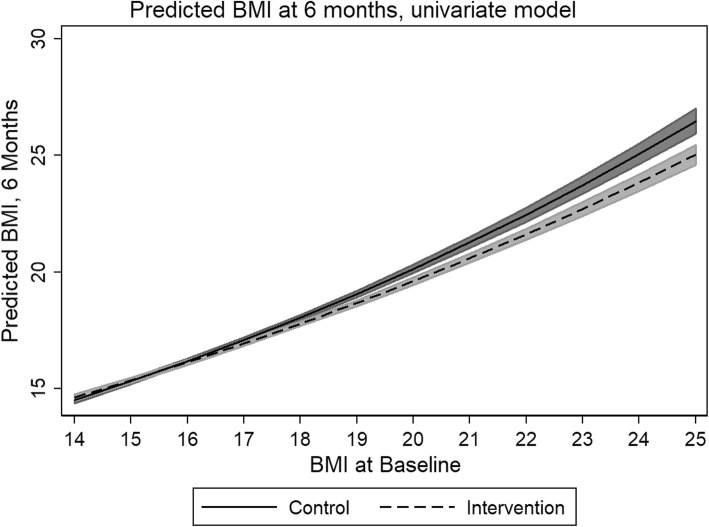
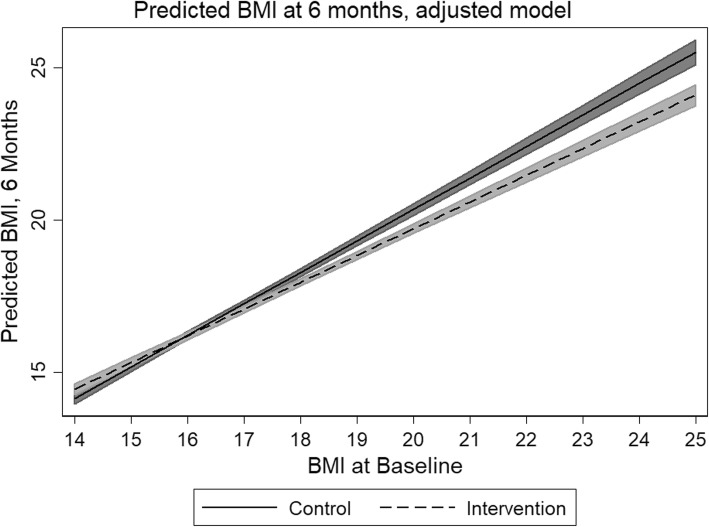
Results: Significant intervention effects were observed for weekday physical activity at home (T1 [P < 0.001] and T2 [P = 0.019]), weekend physical activity (T1 [P < 0.001] and T2 [P < 0.001]), BMI (T2 only [P = 0.020]) and fruit consumption (T1 only [P = 0.036]). Additional analyses revealed that the greatest improvements in physical activity occurred in children from the most socioeconomically deprived schools. No consistent effects on sedentary time, WHtR, or other dietary patterns were observed.
Conclusions: A compulsory health-related homework programme resulted in substantial and consistent increases in children's physical activity - particularly outside of school and on weekends - with limited effects on body size and fruit consumption. Overall, our findings support the integration of compulsory home-focused strategies for improving health behaviours into primary education curricula.
Trial registration: Australian New Zealand Clinical Trials Registry, ACTRN12618000590268 . Registered 17 April 2018.
Keywords: Body size; Child health; Child obesity; Curriculum; Dietary assessment; Education; Intervention; Pedometers.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization . WHO recommendations on child health. Geneva: World Health Organization; 2017.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
