

World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions
- PMID: 31488387
- PMCID: PMC7025029
- DOI: 10.1016/S2214-109X(19)30318-3
World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions
Erratum in
-
Correction to Lancet Glob Health 2019; 7: e1332-45.Lancet Glob Health. 2023 Feb;11(2):e196. doi: 10.1016/S2214-109X(22)00522-8. Epub 2022 Dec 6. Lancet Glob Health. 2023. PMID: 36493797 Free PMC article. No abstract available.
Abstract
Background: To help adapt cardiovascular disease risk prediction approaches to low-income and middle-income countries, WHO has convened an effort to develop, evaluate, and illustrate revised risk models. Here, we report the derivation, validation, and illustration of the revised WHO cardiovascular disease risk prediction charts that have been adapted to the circumstances of 21 global regions.
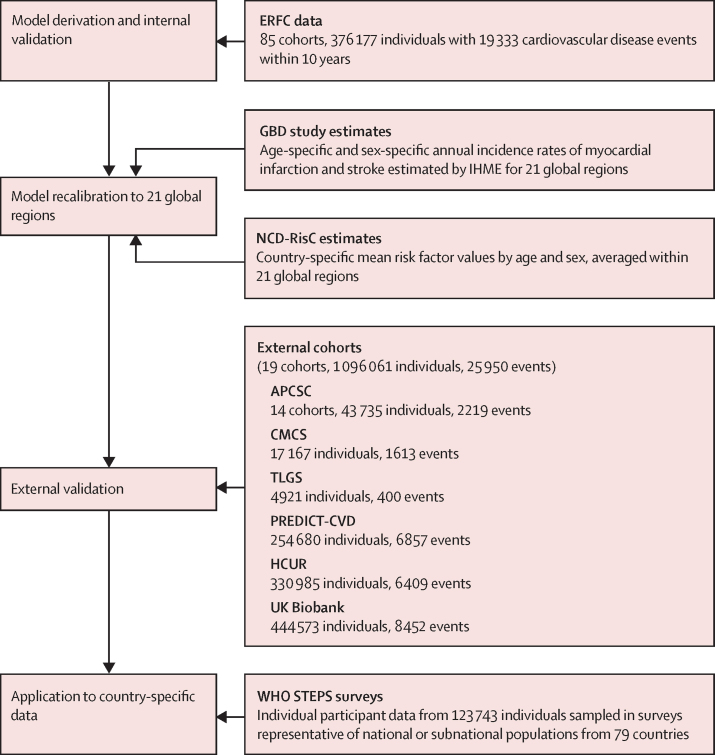
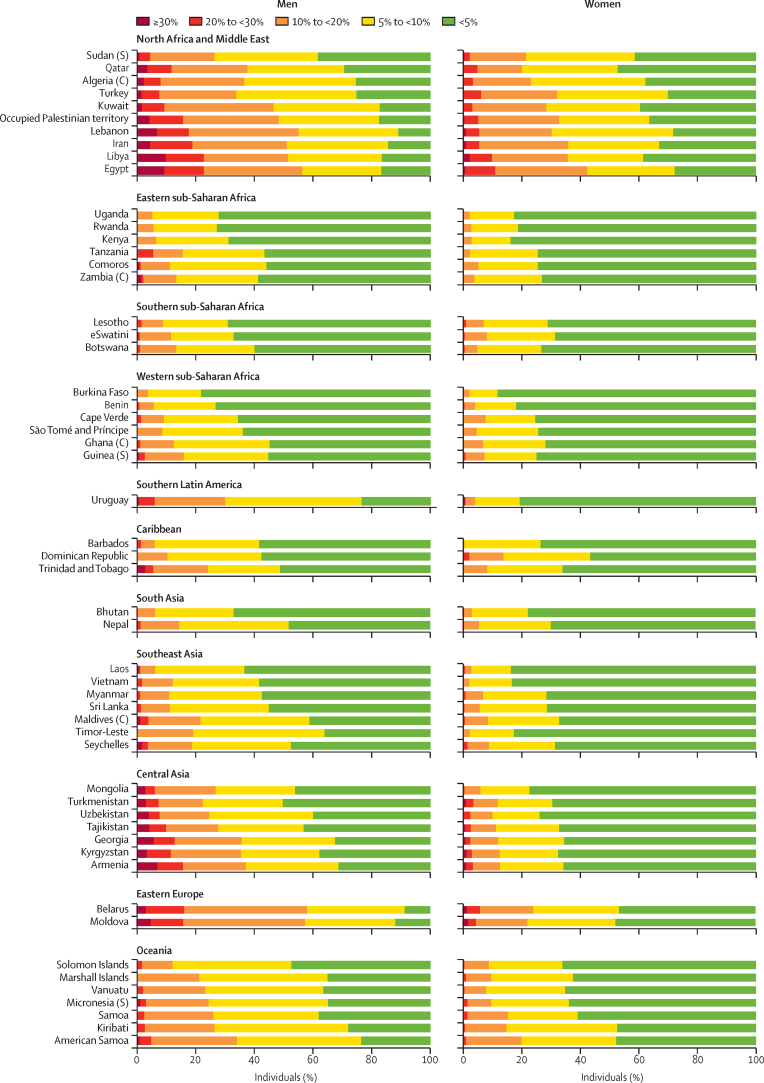
Methods: In this model revision initiative, we derived 10-year risk prediction models for fatal and non-fatal cardiovascular disease (ie, myocardial infarction and stroke) using individual participant data from the Emerging Risk Factors Collaboration. Models included information on age, smoking status, systolic blood pressure, history of diabetes, and total cholesterol. For derivation, we included participants aged 40-80 years without a known baseline history of cardiovascular disease, who were followed up until the first myocardial infarction, fatal coronary heart disease, or stroke event. We recalibrated models using age-specific and sex-specific incidences and risk factor values available from 21 global regions. For external validation, we analysed individual participant data from studies distinct from those used in model derivation. We illustrated models by analysing data on a further 123 743 individuals from surveys in 79 countries collected with the WHO STEPwise Approach to Surveillance.
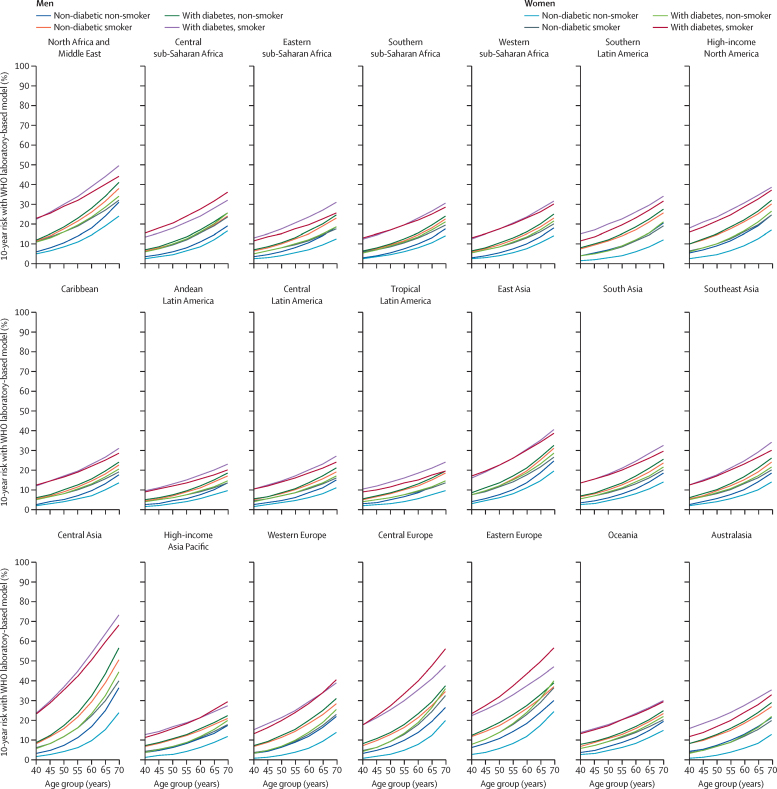
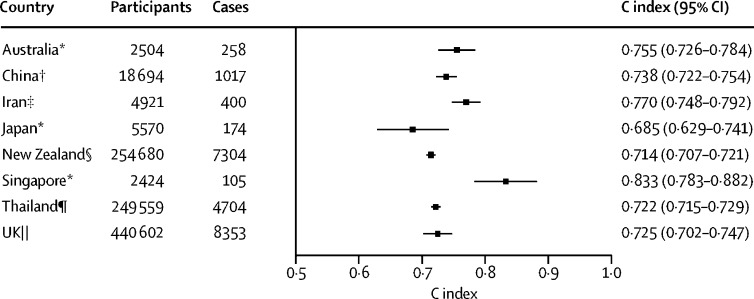
Findings: Our risk model derivation involved 376 177 individuals from 85 cohorts, and 19 333 incident cardiovascular events recorded during 10 years of follow-up. The derived risk prediction models discriminated well in external validation cohorts (19 cohorts, 1 096 061 individuals, 25 950 cardiovascular disease events), with Harrell's C indices ranging from 0·685 (95% CI 0·629-0·741) to 0·833 (0·783-0·882). For a given risk factor profile, we found substantial variation across global regions in the estimated 10-year predicted risk. For example, estimated cardiovascular disease risk for a 60-year-old male smoker without diabetes and with systolic blood pressure of 140 mm Hg and total cholesterol of 5 mmol/L ranged from 11% in Andean Latin America to 30% in central Asia. When applied to data from 79 countries (mostly low-income and middle-income countries), the proportion of individuals aged 40-64 years estimated to be at greater than 20% risk ranged from less than 1% in Uganda to more than 16% in Egypt.
Interpretation: We have derived, calibrated, and validated new WHO risk prediction models to estimate cardiovascular disease risk in 21 Global Burden of Disease regions. The widespread use of these models could enhance the accuracy, practicability, and sustainability of efforts to reduce the burden of cardiovascular disease worldwide.
Funding: World Health Organization, British Heart Foundation (BHF), BHF Cambridge Centre for Research Excellence, UK Medical Research Council, and National Institute for Health Research.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Cardiovascular disease risk prediction models: challenges and perspectives.Lancet Glob Health. 2019 Oct;7(10):e1288-e1289. doi: 10.1016/S2214-109X(19)30365-1. Epub 2019 Sep 2. Lancet Glob Health. 2019. PMID: 31488388 No abstract available.
References
-
- United Nations Transforming our world: the 2030 agenda for sustainable development. 2015. https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E
-
- WHO . World Health Organization; Geneva: 2013. Global action plan for the prevention and control of NCDs 2013–2020.
-
- WHO HEARTS technical package. 2018. https://www.who.int/publications-detail/hearts-technical-package
-
- WHO Package of essential noncommunicable disease interventions in primary health care. https://www.who.int/ncds/management/pen_tools/en/ - PubMed
