

Advanced virtual reality-based rehabilitation of balance and gait in clinical practice
- PMID: 31489154
- PMCID: PMC6710712
- DOI: 10.1177/2040622319868379
Advanced virtual reality-based rehabilitation of balance and gait in clinical practice
Abstract
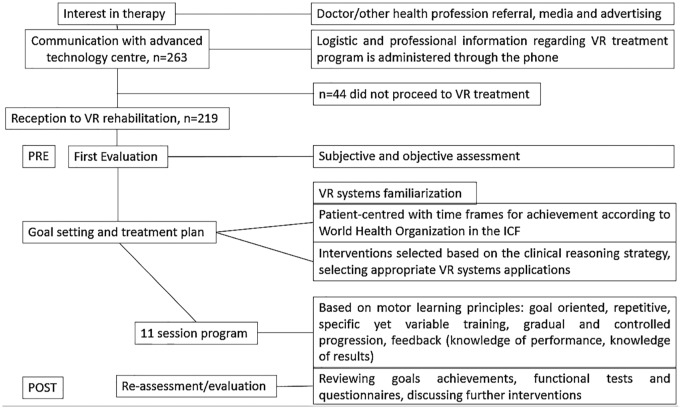
Background: Extensive research shows that virtual reality (VR) enhances motor learning and has advantages in balance and gait rehabilitation of neurological patients. There is still uncertainty, however, as for the practicality and efficacy of VR in long-term clinical routine. The objective of this study was to report on 3 years of clinical practice conducting VR-based rehabilitation of balance and gait in a large medical center.
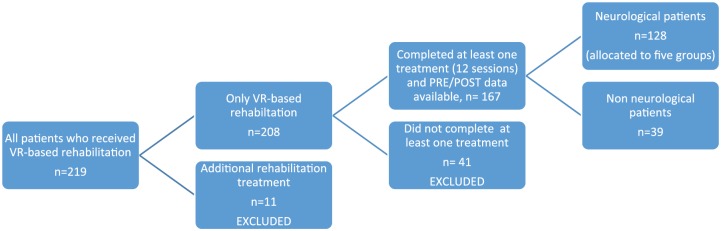
Methods: This retrospective study systematically analyzed clinical records of patients who received VR-based rehabilitation in a large rehabilitation center during 3 years. We evaluated the effect of VR-based rehabilitation treatments on balance and gait, cognitive dual-task load, patient's balance confidence (ABC-scale) and perception of suitability. Patients were either neurological patients, allocated to five groups: Parkinson's disease (PD), poststroke (PS), multiple sclerosis, traumatic brain injury, and 'other conditions', or non-neurological patients.
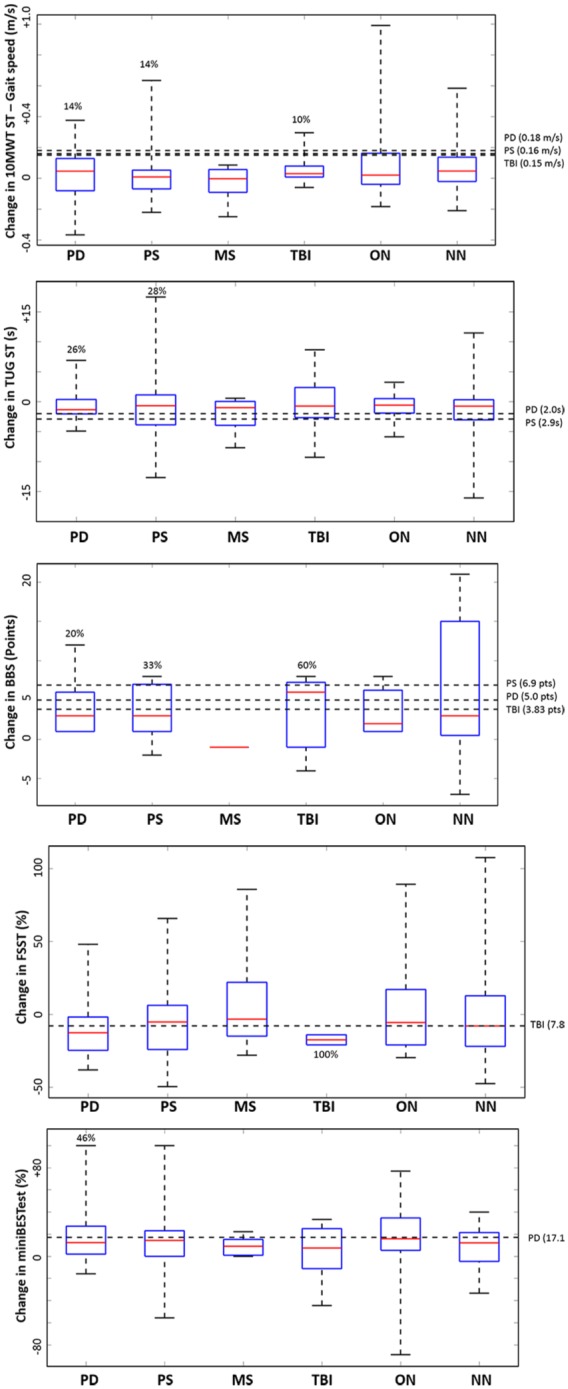
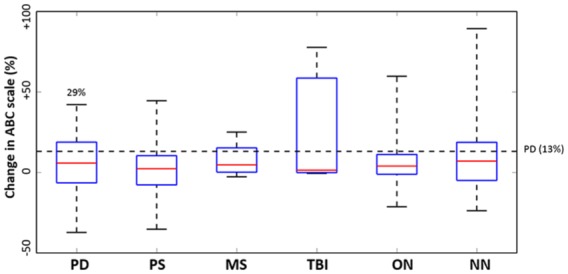
Results: Records of 167 patients were analyzed. The availability of multiple VR systems and environments contributed to highly personalized interventions that tailored specific deficits with therapeutic goals. VR-based rehabilitation significantly improved balance and gait (measured by 10-Meter Walk Test, Timed-Up-and-Go, Berg Balance Scale, and Mini BESTest). Patients with PD and PS decreased dual-task cost while walking. Patients increased balance confidence and deemed VR suitable for rehabilitation.
Conclusions: Our results suggest that VR-based rehabilitation is practicable and effective in clinical routine. Functional measures of balance and gait show significant improvements following VR-based interventions. Clinical approaches should exploit VR advantages for promoting motor learning and motivation. This study serves to aid transition to long-term clinical implementation of VR.
Keywords: Parkinson’s disease; brain injury; multiple sclerosis; posture; rehabilitation; stroke; virtual reality; walking.
Conflict of interest statement
Conflict of interest statement: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Kasser SL, Jacobs JV, Ford Met al. Effects of balance-specific exercises on balance, physical activity and quality of life in adults with multiple sclerosis: a pilot investigation. Disabil Rehabil 2015; 37: 2238–2249. - PubMed
-
- Michael KM, Allen JK, Macko RF. Reduced ambulatory activity after stroke: the role of balance, gait, and cardiovascular fitness. Arch Phys Med Rehabil 2005; 86: 1552–1556. - PubMed
LinkOut - more resources
Full Text Sources
