

Perioperative impact of liver venous deprivation compared with portal venous embolization in patients undergoing right hepatectomy: preliminary results from the pioneer center
- PMID: 31489302
- PMCID: PMC6700017
- DOI: 10.21037/hbsn.2019.07.06
Perioperative impact of liver venous deprivation compared with portal venous embolization in patients undergoing right hepatectomy: preliminary results from the pioneer center
Abstract
Background: Preoperative portal vein embolization (PVE) is currently the standard technique used routinely to increase the size of the future remnant liver (FRL) before major hepatectomies. The degree of hypertrophy (DH) is approximatively 10% and requires on average six weeks. ALPPS is faster and achieves a good DH but with a higher morbidity and mortality. One method recently proposed to increase the FRL is liver venous deprivation (LVD), but its clinical and operative impact is still unknown. The aim of this study is to compare intra- and postoperative morbidity/mortality and the histological evaluation of the liver parenchyma between PVE and LVD in patients undergoing anatomic right hepatectomy.
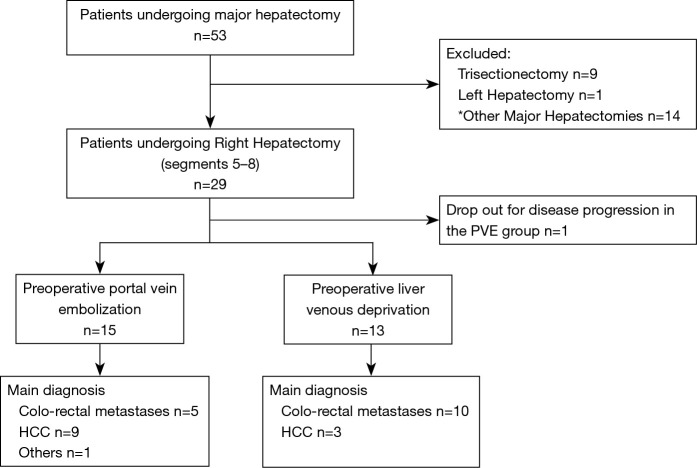
Methods: Fifty-three consecutive patients undergoing PVE and LVD before a major hepatectomy were retrospectively analysed between 2015 and 2017. In order to reduce the bias, only potential standard right hepatectomies were selected. Surgical resections and the radiologic procedures were performed by the same Institution. Intra-operative parameters (transfusions, perfusions, bleeding, operative time), postoperative complications (Clavien-Dindo and ISGLS criteria), and histological findings were compared.
Results: To induce FRL growth 16 patients underwent PVE and 13 LVD. One patient of the PVE group was not resected due to peritoneal metastases. Surgery was performed for hepatocellular carcinoma (PVE =9, LVD =3), metastases (PVE =5, LVD =10), or others diseases (PVE =2, LVD =0). Per- and post-operative morbidity/mortality rates after PVE and LVD procedures were null. No differences between the two groups were found in terms of intraoperative bleeding (median: 550 vs. 1,200 mL; P=0.36), hepatic pedicle clamping (5 vs. 3 patients; P=0.69), intraoperative red blood cells transfusions (median: 622 vs. 594; P=0.42) and operative time (median: 270 vs. 330 min; P=0.34). Post-operative course was similar when comparing both medical and surgical complications in the two arms (PVE n=7, LVD n=10, P=0.1). Major complications (Clavien-Dindo ≥ IIIa) occurred in 3 patients undergoing PVE and in 1 patient of the LVD group (P=0.6). No difference in biliary leak (P=0.1), haemorrhage (P=0.2) and liver failure (P=0.64) was found. One cirrhotic patient in the group of PVE died of post-operative liver failure due to left portal vein thrombosis. Although we experienced a more marked liver damage when assessing on neoplastic liver parenchyma, no statistical difference was observed in terms of atrophy (P=0.19), necrosis (P=0.5), hemorrhage (P=0.42) and sinusoidal dilatation (P=0.69).
Conclusions: Despite the limitations of our study, to our knowledge this is the first report to compare the two techniques LVD is a promising and safe procedure to induce a fast FRL hypertrophy, showing similar mortality/morbidity rates during and after surgery compared to PVE.
Keywords: Liver venous deprivation (LVD); hepatectomy; liver failure; portal embolization.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Comment in
-
Optimizing future remnant liver prior to major hepatectomies: increasing volume while decreasing morbidity and mortality.Hepatobiliary Surg Nutr. 2020 Apr;9(2):215-218. doi: 10.21037/hbsn.2019.10.24. Hepatobiliary Surg Nutr. 2020. PMID: 32355683 Free PMC article. No abstract available.
-
New evidence for liver venous deprivation: safety and feasibility for extended liver resections.Ann Transl Med. 2020 Oct;8(19):1259. doi: 10.21037/atm-20-3057. Ann Transl Med. 2020. PMID: 33178791 Free PMC article. No abstract available.
References
-
- Makuuchi M, Thai BL, Takayasu K, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990;107:521-7. - PubMed
-
- Yamashita S, Sakamoto Y, Yamamoto S, et al. Efficacity of preoperative portal vein embolization among patients with hepatocellular carcinoma, biliary tract cancer and colorectal liver metastases: a comparative study based on single center experience of 319 cases. Ann Surg Oncol 2017;24:1557-68. 10.1245/s10434-017-5800-z - DOI - PubMed
LinkOut - more resources
Full Text Sources