

A direct endoscopic approach for left-sided infrarenal para-aortic lymphadenectomy immediately after hysterectomy for endometrial cancer treatment: left dome formation (LDF)
- PMID: 31489501
- PMCID: PMC7326799
- DOI: 10.1007/s00464-019-07103-3
A direct endoscopic approach for left-sided infrarenal para-aortic lymphadenectomy immediately after hysterectomy for endometrial cancer treatment: left dome formation (LDF)
Abstract
Background: Endoscopic surgery for infrarenal para-aortic lymphadenectomy has been widely accepted. Two major approaches, "transperitoneal" and "extraperitoneal", are generally used; however, they have several disadvantages. A "transperitoneal" approach to the left para-aortic region is usually indirect, often performed after wide extension of the right para-aortic region. An "extraperitoneal" approach is unsuitable when a peritoneal tear exists after a prior surgical procedure such as hysterectomy. Here, we propose a modified transperitoneal technique, "Left dome formation (LDF)," which directly provides a surgical field for left infrarenal para-aortic lymphadenectomy even after hysterectomy.
Methods: The LDF procedure comprised three processes: (1) setting, (2) dissection of inframesenteric lymph nodes (step 1), and (3) dissection of infrarenal lymph nodes (step 2).
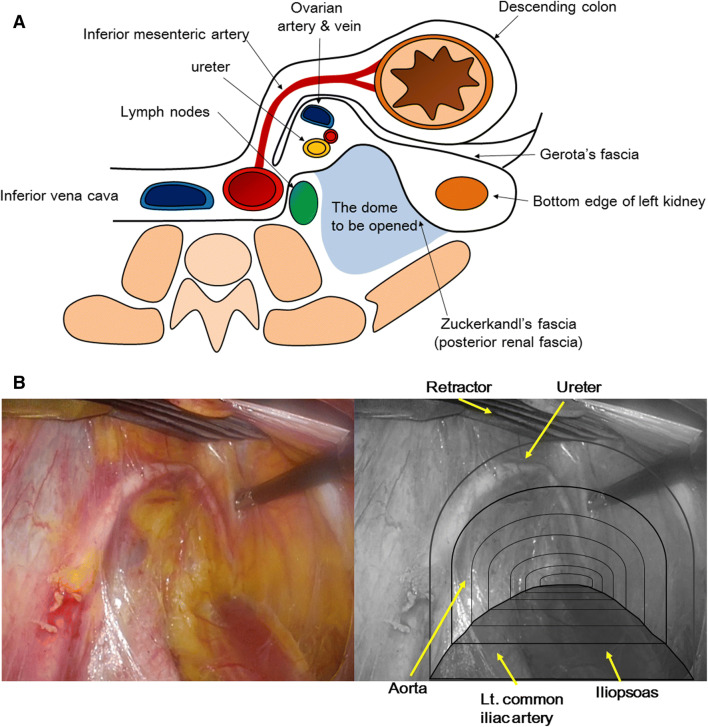
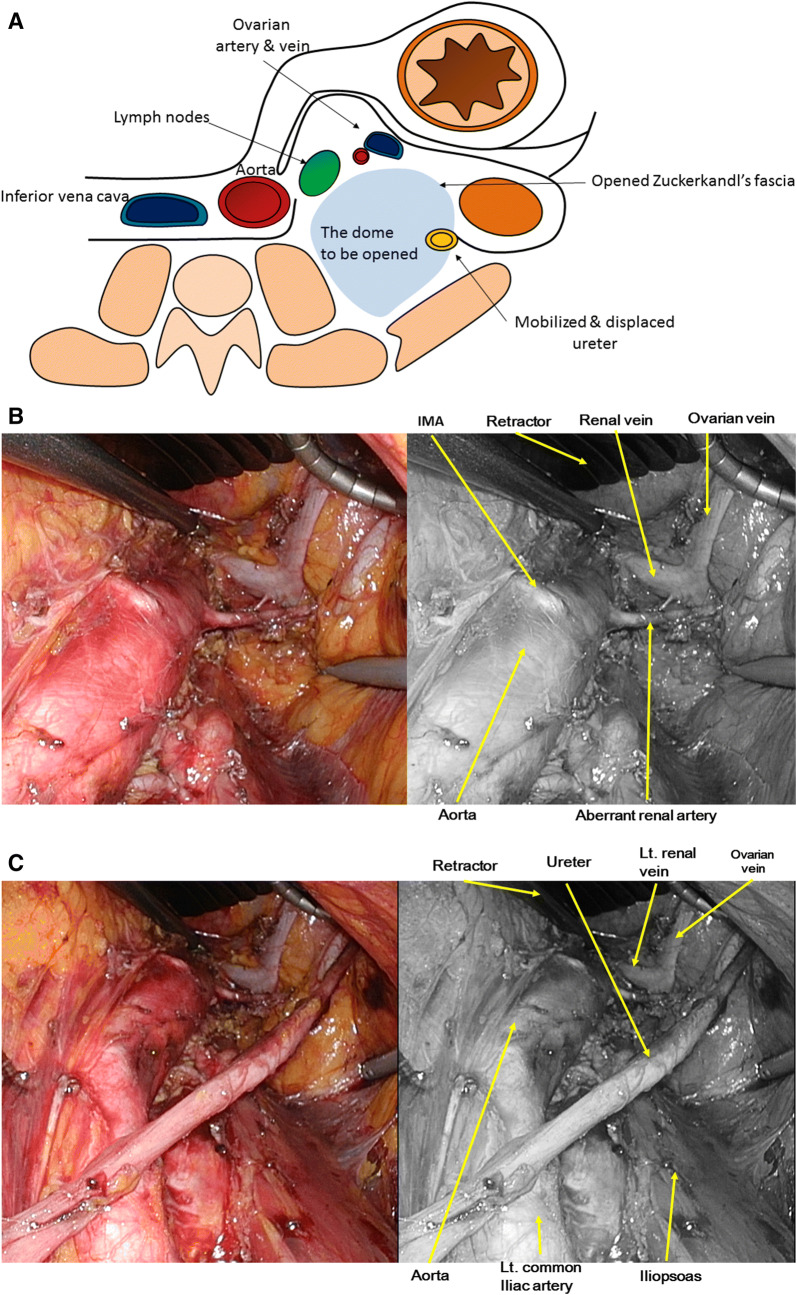
Setting: two trocars were added 4 cm bilateral to the low-mid abdominal trocar that was used in prior hysterectomy. Step 1: The posterior layer of the renal fascia along with the left ureter and left ovarian vessel were separated from the left common iliac artery and iliopsoas. Left inframesentric nodes were removed from the surgical field. Step 2: The left ureter was isolated from the posterior renal fascia, and the dome was expanded cranially to the left renal vein, with the ovarian vein always visualizable at the dome ceiling. Left infrarenal nodes were removed.
Results: We applied LDF to ten endometrial cancer patients, recommended for additional dissection of para-aortic nodes based on intraoperative evaluation using the laparoscopically removed uterus. The operative time and number of removed lymph nodes in Step 1 and Step 2 were 28.8 (20-49) min and 5.3 (2-10) and 54.6 (52-70) min and 6.5 (1-11), respectively. Blood loss was below 50 ml. No serious organ injury occurred during procedures.
Conclusion: Since the left ureter is always observable, LDF procedure facilitates effective surgery to overcome the anatomical complexity of the left para-aortic region and is potentially useful for sentinel node sampling.
Keywords: Direct access; Dome formation; Endometrial cancer; Left-sided infrarenal para-aortic lymphadenectomy; Sentinel node sampling.
Conflict of interest statement
Drs. Y. Mizumoto, J. Iwadare, K. Nakade, T. Obata, T. Matsumoto, K. Kagami, T. Iizuka, A. Matsuoka, M. Ono, M. Nakamura, and H. Fujiwara have no conflicts of interest or financial ties to disclose.
Figures

References
-
- Tanaka T, Terai Y, Ono YJ, Fujiwara S, Tanaka Y, Sasaki H, Tsunetoh S, Kanemura M, Yamamoto K, Yamada T, Ohmichi M. Preoperative MRI and intraoperative frozen section diagnosis of myometrial invation in patients with endometrial cancer. Int J Gynecol Cancer. 2015;25(5):879–883. doi: 10.1097/IGC.0000000000000470. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
