

Tumor necrosis factor-mediated disposition of infliximab in ulcerative colitis patients
- PMID: 31489538
- PMCID: PMC6868113
- DOI: 10.1007/s10928-019-09652-5
Tumor necrosis factor-mediated disposition of infliximab in ulcerative colitis patients
Abstract
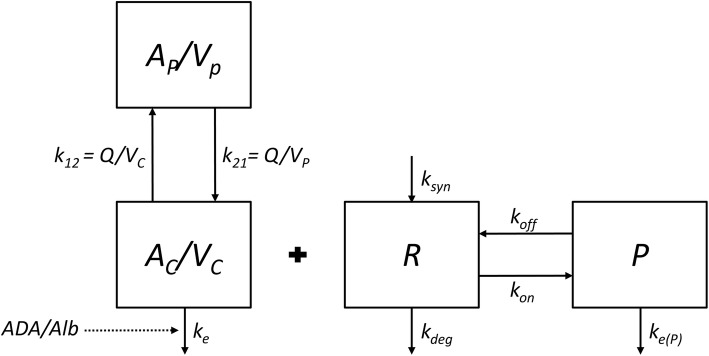
Ulcerative Colitis (UC) is an inflammatory bowel disease typically affecting the colon. Patients with active UC have elevated tumor necrosis factor (TNF) concentrations in serum and colonic tissue. Infliximab is a monoclonal antibody directed against TNF and binds with high affinity. Target-mediated drug disposition (TMDD) is reported for monoclonal antibodies meaning that their pharmacokinetics are affected by high target affinity. Here, a TMDD model is proposed to describe the interaction between infliximab and TNF in UC patients. Data from 20 patients with moderate to severe UC was used. Patients received standard infliximab induction therapy (5 mg kg-1) at week 0, followed by infusions at week 2 and 6. IFX, anti-drug antibodies and TNF serum concentrations were measured at day 0 (1 h after infusion), 1, 4, 7, 11, 14, 18, 21, 28 and 42. A binding model, TMDD model, and a quasi-steady state (QSS) approximation were evaluated using nonlinear mixed effects modeling (NONMEM). A two-compartment model best described the concentration-time profiles of infliximab. Typical clearance of infliximab was 0.404 L day-1 and increased with the presence of anti-drug antibodies and with lower albumin concentrations. The TMDD-QSS model best described the pharmacokinetic and pharmacodynamics data. Estimate for TNF baseline (Bmax was 19.8 pg mL-1 and the dissociation constant (Kss) was 13.6 nM. This model could eventually be used to investigate the relationship between suppression of TNF and the response to IFX therapy.
Keywords: Infliximab; Monoclonal antibody; Target-mediated drug disposition; Ulcerative colitis.
Figures



Similar articles
-
Generalized Pyoderma Gangrenosum Associated with Ulcerative Colitis: Successful Treatment with Infliximab and Azathioprine.Acta Dermatovenerol Croat. 2016 Apr;24(1):83-5. Acta Dermatovenerol Croat. 2016. PMID: 27149138
-
Elevation of PRKCDBP, a novel transcriptional target of TNF-α, and its downregulation by infliximab in patients with ulcerative colitis.Dig Dis Sci. 2014 Dec;59(12):2947-57. doi: 10.1007/s10620-014-3282-4. Epub 2014 Jul 23. Dig Dis Sci. 2014. PMID: 25052149
-
Loss of Infliximab Into Feces Is Associated With Lack of Response to Therapy in Patients With Severe Ulcerative Colitis.Gastroenterology. 2015 Aug;149(2):350-5.e2. doi: 10.1053/j.gastro.2015.04.016. Epub 2015 Apr 25. Gastroenterology. 2015. PMID: 25917786 Clinical Trial.
-
Therapeutic Drug Monitoring of Golimumab in the Treatment of Ulcerative Colitis.Pharm Res. 2017 Aug;34(8):1556-1563. doi: 10.1007/s11095-017-2150-2. Epub 2017 Apr 3. Pharm Res. 2017. PMID: 28374338 Review.
-
A review of infliximab use in ulcerative colitis.Clin Ther. 2008 Feb;30(2):223-30. doi: 10.1016/j.clinthera.2008.02.014. Clin Ther. 2008. PMID: 18343261 Review.
Cited by
-
What to do when traditional rescue therapies fail in acute severe ulcerative colitis.Intest Res. 2024 Oct;22(4):397-413. doi: 10.5217/ir.2024.00003. Epub 2024 May 16. Intest Res. 2024. PMID: 38749658 Free PMC article. Review.
-
Infliximab Efficacy May Be Linked to Full TNF-α Blockade in Peripheral Compartment-A Double Central-Peripheral Target-Mediated Drug Disposition (TMDD) Model.Pharmaceutics. 2021 Nov 1;13(11):1821. doi: 10.3390/pharmaceutics13111821. Pharmaceutics. 2021. PMID: 34834236 Free PMC article.
-
Qingre Xingyu recipe exerts inhibiting effects on ulcerative colitis development by inhibiting TNFα/NLRP3/Caspase-1/IL-1β pathway and macrophage M1 polarization.Cell Death Discov. 2023 Mar 8;9(1):84. doi: 10.1038/s41420-023-01361-w. Cell Death Discov. 2023. PMID: 36890151 Free PMC article.
-
Upper gut heat shock proteins HSP70 and GRP78 promote insulin resistance, hyperglycemia, and non-alcoholic steatohepatitis.Nat Commun. 2022 Dec 13;13(1):7715. doi: 10.1038/s41467-022-35310-5. Nat Commun. 2022. PMID: 36513656 Free PMC article.
-
Local depletion of large molecule drugs due to target binding in tissue interstitial space.CPT Pharmacometrics Syst Pharmacol. 2024 Dec;13(12):2068-2086. doi: 10.1002/psp4.13262. Epub 2024 Nov 12. CPT Pharmacometrics Syst Pharmacol. 2024. PMID: 39530200 Free PMC article. Review.
References
-
- Komatsu M, Kobayashi D, Saito K, Furuya D, Yagihashi A, Araake H, Tsuji N, Sakamaki S, Niitsu Y, Watanabe N. Tumor necrosis factor in serum of patients with inflammatory bowel disease as measured by a highly sensitive immuno-PCR. Clin Chem. 2001;47:1297–1301. - PubMed
-
- Martínez-Borra J, López-Larrea C, González S, Fuentes D, Dieguez A, Deschamps EM, Pérez-Pariente JM, López-Vázquez A, De Francisco R, Rodrigo L. High serum tumor necrosis factor-α levels are associated with lack of response to infliximab in fistulizing Crohn’s disease. Am J Gastroenterol. 2002;97(9):2350–2356. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
