

Diabetes in relation to Barrett's esophagus and adenocarcinomas of the esophagus: A pooled study from the International Barrett's and Esophageal Adenocarcinoma Consortium
- PMID: 31490550
- PMCID: PMC7001889
- DOI: 10.1002/cncr.32444
Diabetes in relation to Barrett's esophagus and adenocarcinomas of the esophagus: A pooled study from the International Barrett's and Esophageal Adenocarcinoma Consortium
Abstract
Background: Diabetes is positively associated with various cancers, but its relationship with tumors of the esophagus/esophagogastric junction remains unclear.
Methods: Data were harmonized across 13 studies in the International Barrett's and Esophageal Adenocarcinoma Consortium, comprising 2309 esophageal adenocarcinoma (EA) cases, 1938 esophagogastric junction adenocarcinoma (EGJA) cases, 1728 Barrett's esophagus (BE) cases, and 16,354 controls. Logistic regression was used to estimate study-specific odds ratios (ORs) and 95% CIs for self-reported diabetes in association with EA, EGJA, and BE. Adjusted ORs were then combined using random-effects meta-analysis.
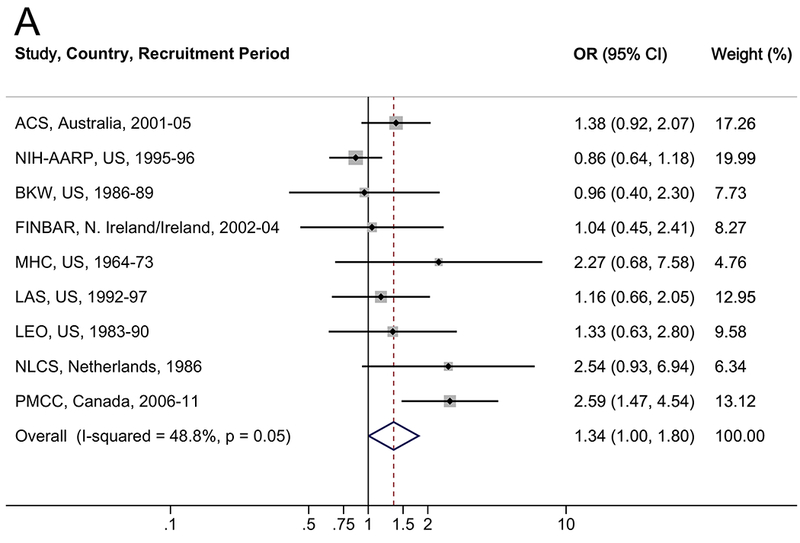
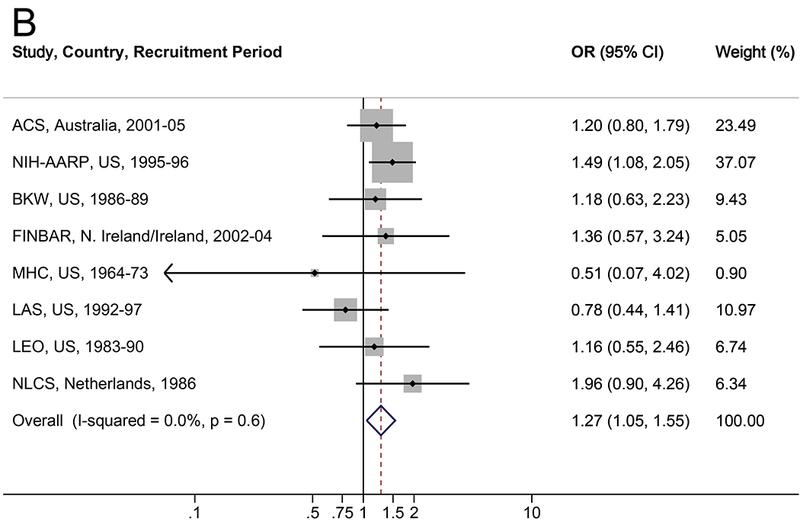
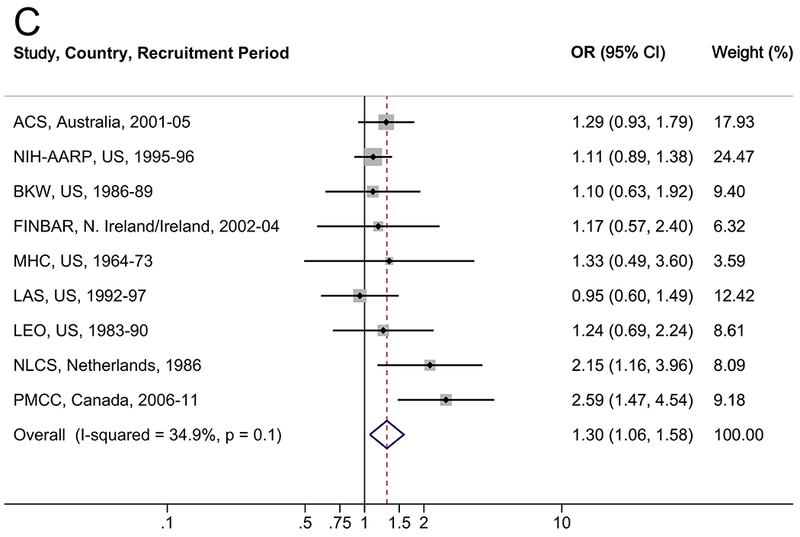
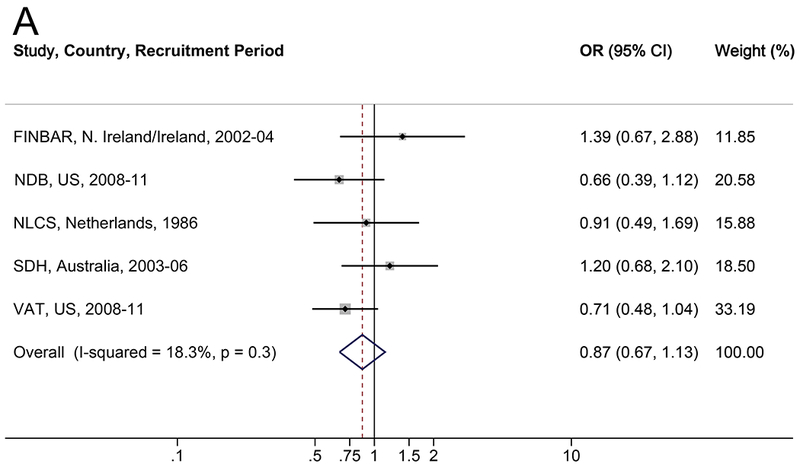
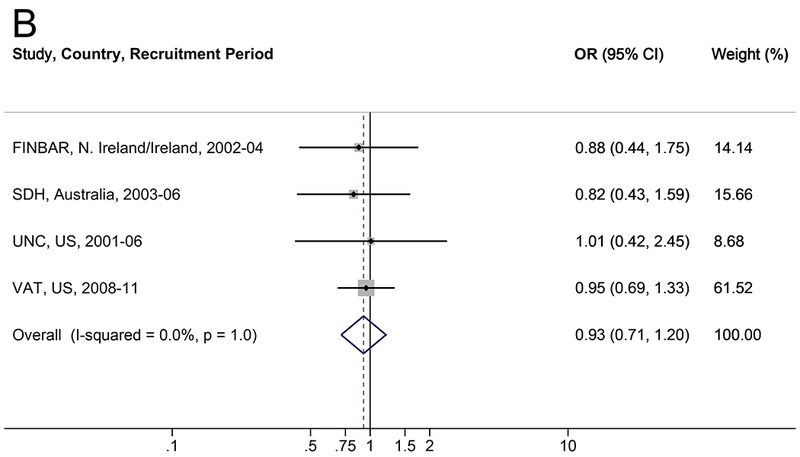
Results: Diabetes was associated with a 34% increased risk of EA (OR, 1.34; 95% CI, 1.00-1.80; I2 = 48.8% [where 0% indicates no heterogeneity, and larger values indicate increasing heterogeneity between studies]), 27% for EGJA (OR, 1.27; 95% CI, 1.05-1.55; I2 = 0.0%), and 30% for EA/EGJA combined (OR, 1.30; 95% CI, 1.06-1.58; I2 = 34.9%). Regurgitation symptoms modified the diabetes-EA/EGJA association (P for interaction = .04) with a 63% increased risk among participants with regurgitation (OR, 1.63; 95% CI, 1.19-2.22), but not among those without regurgitation (OR, 1.03; 95% CI, 0.74-1.43). No consistent association was found between diabetes and BE.
Conclusions: Diabetes was associated with increased EA and EGJA risk, which was confined to individuals with regurgitation symptoms. Lack of an association between diabetes and BE suggests that diabetes may influence progression of BE to cancer.
Keywords: Barrett esophagus; diabetes; epidemiology; esophageal adenocarcinoma; meta-analysis.
© 2019 American Cancer Society.
Conflict of interest statement
Figures
References
-
- Simard EP, Ward EM, Siegel R, Jemal A. Cancers with increasing incidence trends in the United States: 1999 through 2008. CA Cancer J Clin. 2012;62: 118–128. - PubMed
-
- Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005;97: 142–146. - PubMed
-
- Islami F, DeSantis CE, Jemal A. Incidence Trends of Esophageal and Gastric Cancer Subtypes by Race, Ethnicity, and Age in the United States, 1997–2014. Clin Gastroenterol Hepatol. 2019;17: 429–439. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF, Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83: 2049–2053. - PubMed
-
- Wijnhoven BP, Siersema PD, Hop WC, van Dekken H, Tilanus HW. Adenocarcinomas of the distal oesophagus and gastric cardia are one clinical entity. Rotterdam Oesophageal Tumour Study Group. Br J Surg. 1999;86: 529–535. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
- U01 CA199336/CA/NCI NIH HHS/United States
- U54 CA163059/CA/NCI NIH HHS/United States
- R01 CA001833/CA/NCI NIH HHS/United States
- R01 DK063616/DK/NIDDK NIH HHS/United States
- R01 CA109193/CA/NCI NIH HHS/United States
- K23DK059311/NH/NIH HHS/United States
- ZIA CP010220/ImNIH/Intramural NIH HHS/United States
- K08DK002697/NH/NIH HHS/United States
- R01CA116845/NH/NIH HHS/United States
- K23DK079291/NH/NIH HHS/United States
- R01CA059636/NH/NIH HHS/United States
- R01CA030022/NH/NIH HHS/United States
- I01 CX000899/CX/CSRD VA/United States
- U01CA199336/NH/NIH HHS/United States
- R01 CA116845/CA/NCI NIH HHS/United States
- K08 DK002697/DK/NIDDK NIH HHS/United States
- R37CA041530/NH/NIH HHS/United States
- R01DK063616/NH/NIH HHS/United States
- U01 CA057949/CA/NCI NIH HHS/United States
- R01 CA030022/CA/NCI NIH HHS/United States
- U54CA163059/NH/NIH HHS/United States
- K23 DK079291/DK/NIDDK NIH HHS/United States
- R01CA001833/NH/NIH HHS/United States
- P30 DK056338/DK/NIDDK NIH HHS/United States
- U01CA057949/NH/NIH HHS/United States
- R01CA109193/NH/NIH HHS/United States
- K23 DK059311/DK/NIDDK NIH HHS/United States
- K07 CA222060/CA/NCI NIH HHS/United States
