

Antibiotics-Driven Gut Microbiome Perturbation Alters Immunity to Vaccines in Humans
- PMID: 31491384
- PMCID: PMC6750738
- DOI: 10.1016/j.cell.2019.08.010
Antibiotics-Driven Gut Microbiome Perturbation Alters Immunity to Vaccines in Humans
Abstract
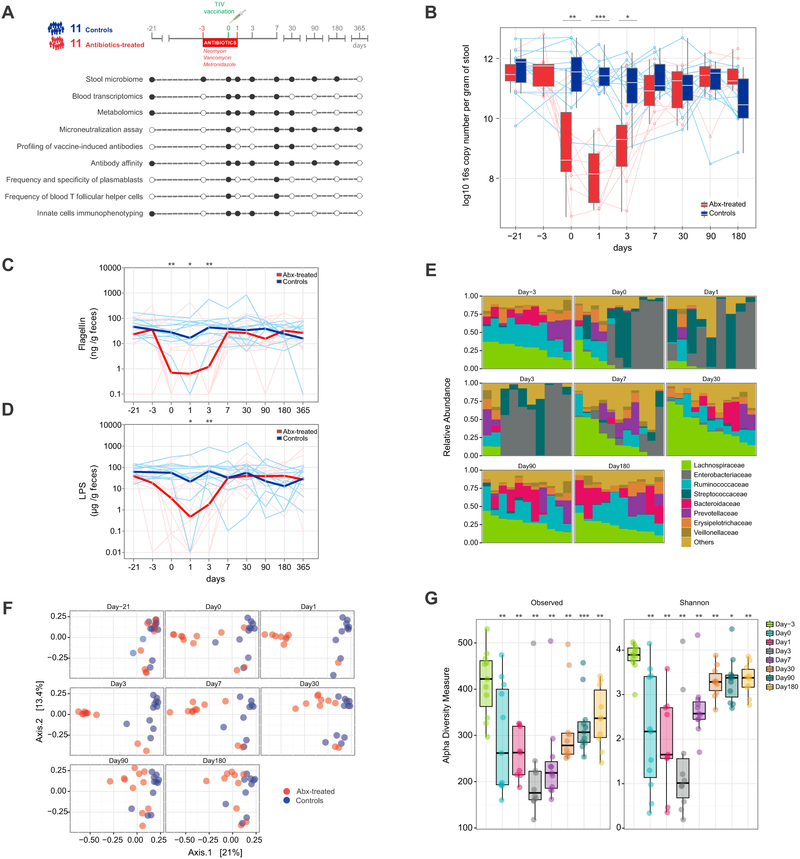
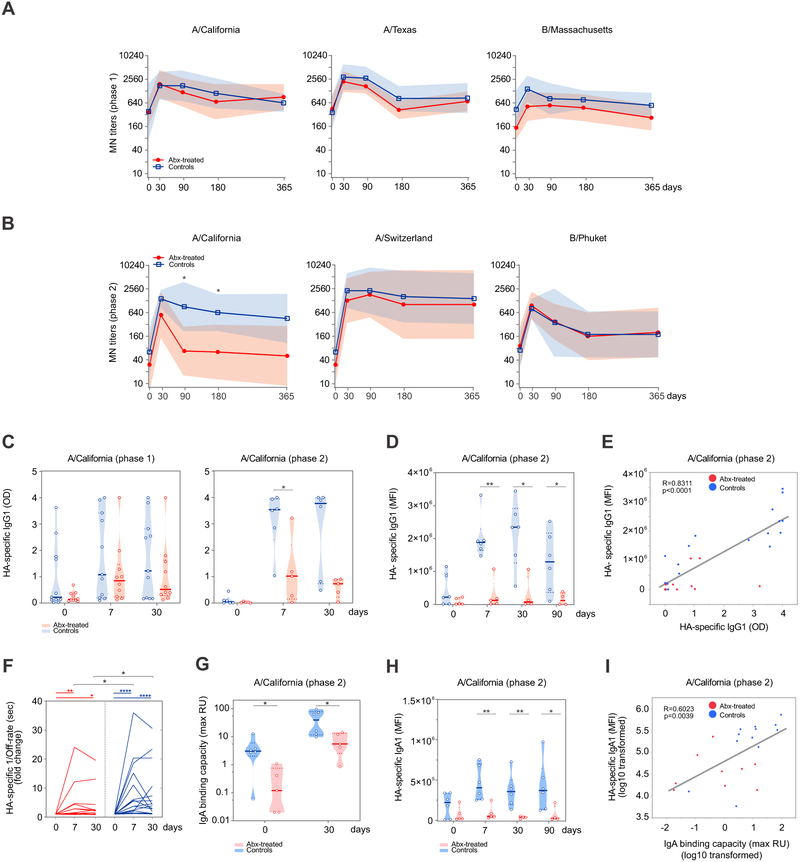
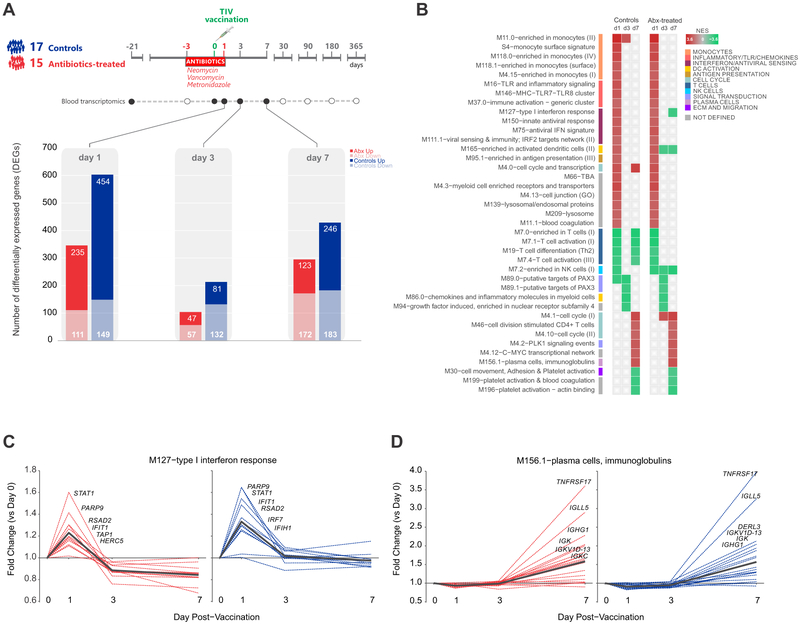
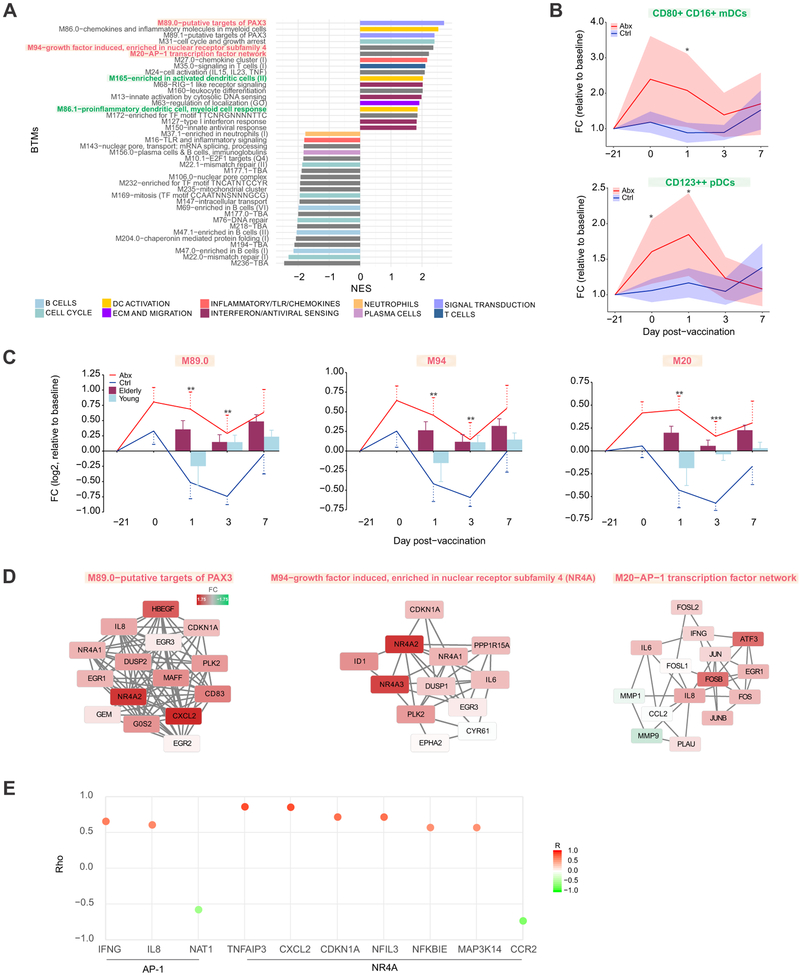
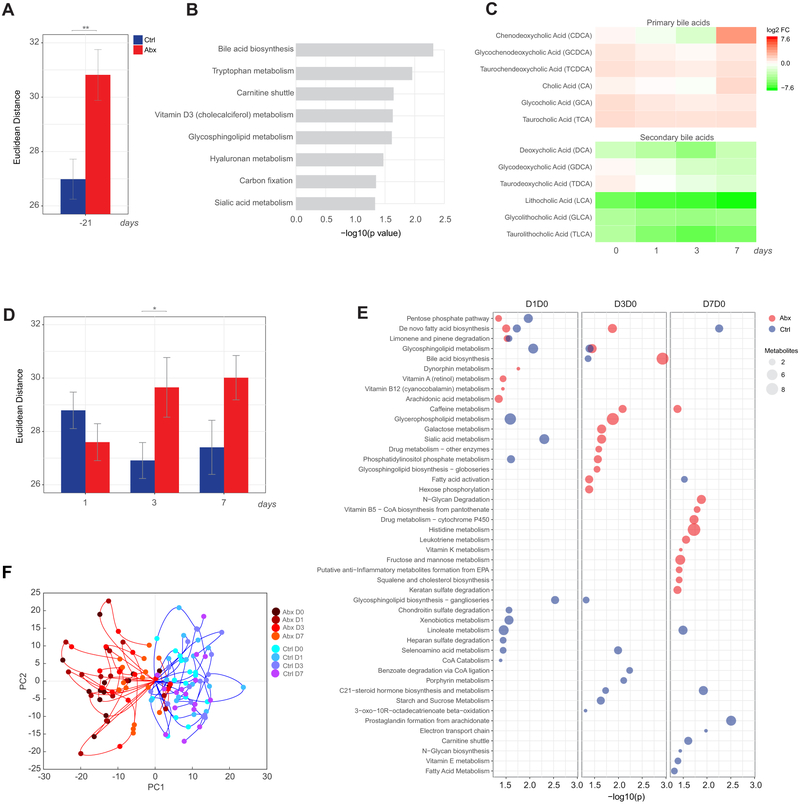
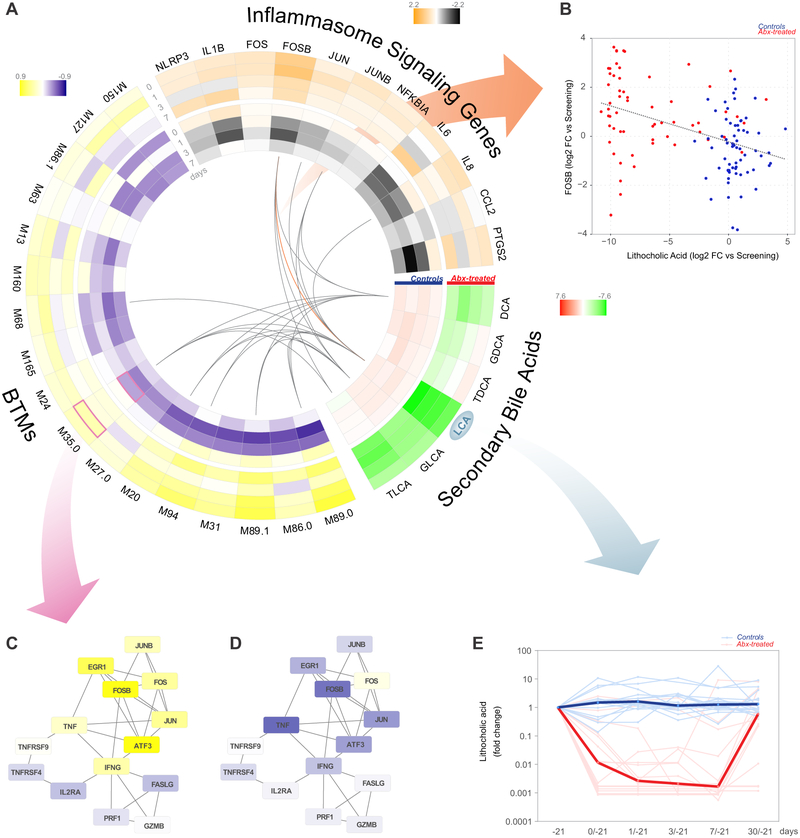
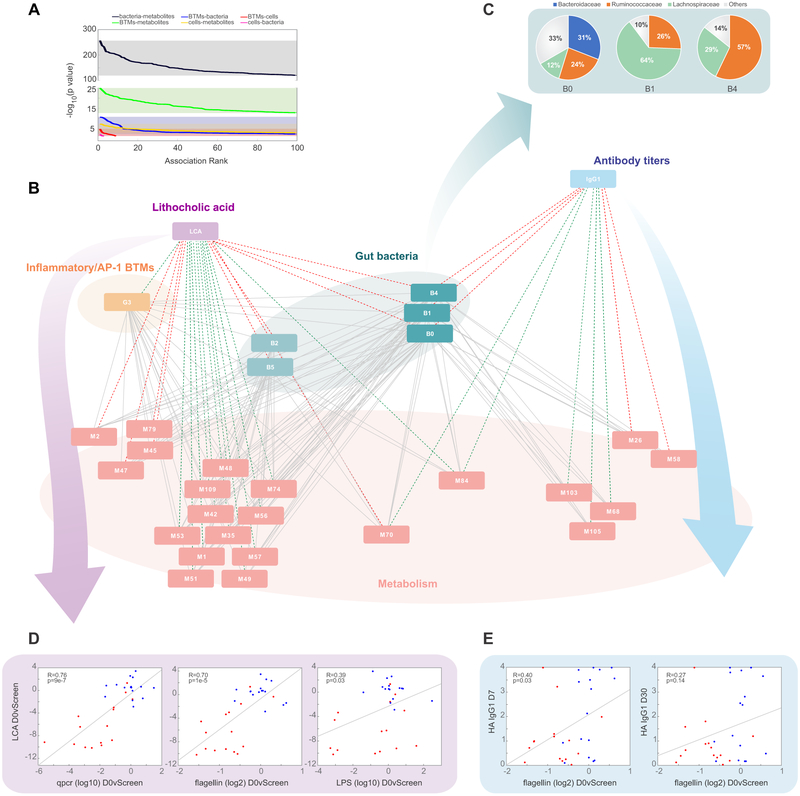
Emerging evidence indicates a central role for the microbiome in immunity. However, causal evidence in humans is sparse. Here, we administered broad-spectrum antibiotics to healthy adults prior and subsequent to seasonal influenza vaccination. Despite a 10,000-fold reduction in gut bacterial load and long-lasting diminution in bacterial diversity, antibody responses were not significantly affected. However, in a second trial of subjects with low pre-existing antibody titers, there was significant impairment in H1N1-specific neutralization and binding IgG1 and IgA responses. In addition, in both studies antibiotics treatment resulted in (1) enhanced inflammatory signatures (including AP-1/NR4A expression), observed previously in the elderly, and increased dendritic cell activation; (2) divergent metabolic trajectories, with a 1,000-fold reduction in serum secondary bile acids, which was highly correlated with AP-1/NR4A signaling and inflammasome activation. Multi-omics integration revealed significant associations between bacterial species and metabolic phenotypes, highlighting a key role for the microbiome in modulating human immunity.
Keywords: antibodies; bile acids; gene expression profiling; immunology; influenza; metabolomics; microbiota; systems biology; systems vaccinology; vaccines.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Antibiotics can impede flu vaccines.Nat Rev Immunol. 2019 Nov;19(11):663. doi: 10.1038/s41577-019-0227-3. Nat Rev Immunol. 2019. PMID: 31551570 No abstract available.
References
-
- Agus A, Planchais J, and Sokol H (2018). Gut Microbiota Regulation of Tryptophan Metabolism in Health and Disease. Cell Host Microbe 23, 716–724. - PubMed
-
- Bray JR, and Curtis JT (1957). An Ordination of the Upland Forest Communities of Southern Wisconsin. Ecol Monogr 27, 326–349.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
