

Domesticating the foreign body response: Recent advances and applications
- PMID: 31491445
- PMCID: PMC6774350
- DOI: 10.1016/j.addr.2019.08.010
Domesticating the foreign body response: Recent advances and applications
Abstract
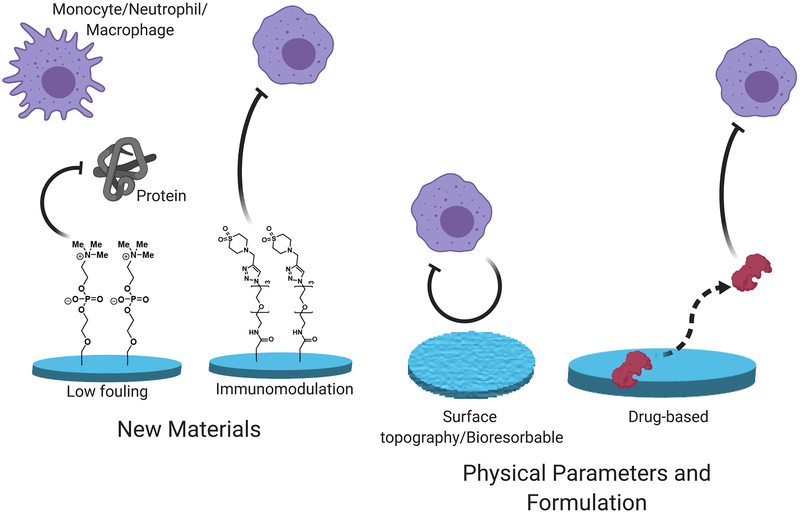
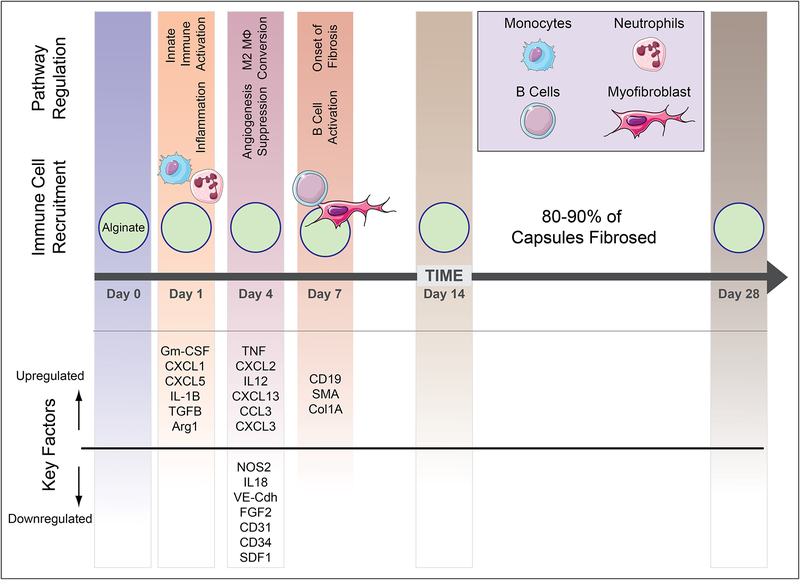
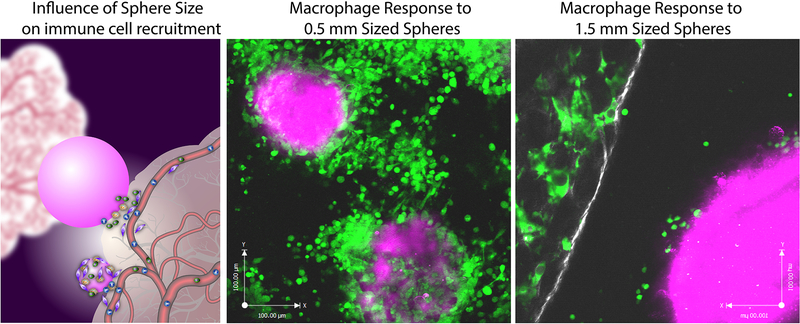
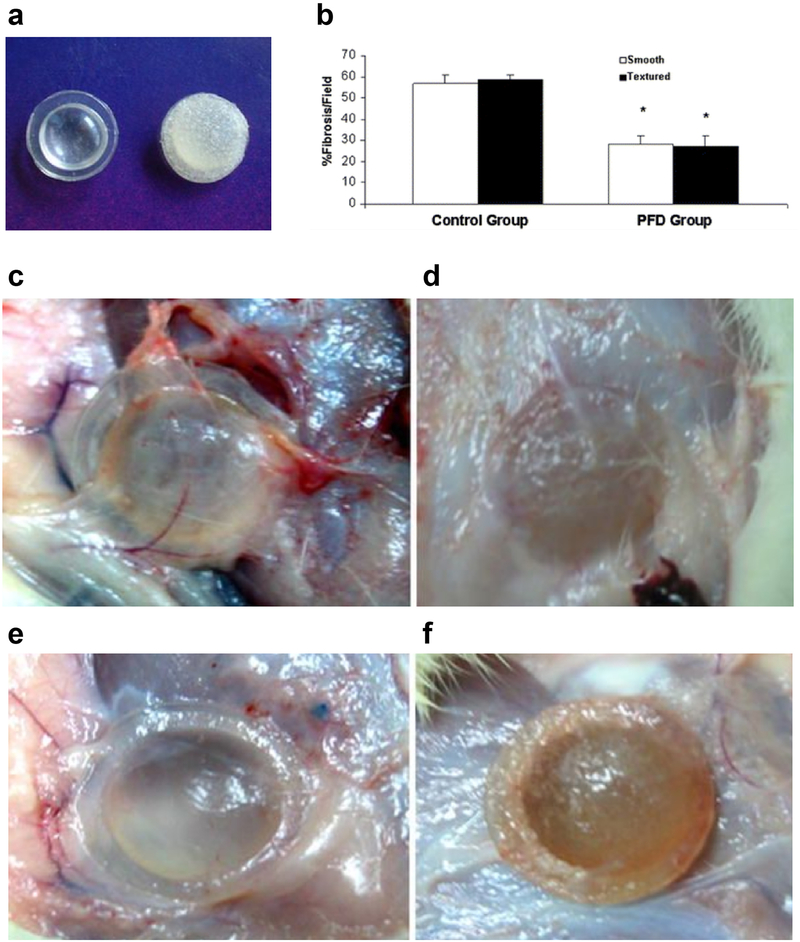
The foreign body response is an immunological process that leads to the rejection of implanted devices and presents a fundamental challenge to their performance, durability, and therapeutic utility. Recent advances in materials development and device design are now providing strategies to overcome this immune-mediated reaction. Here, we briefly review our current mechanistic understanding of the foreign body response and highlight new anti-FBR technologies from this decade that have been applied successfully in biomedical applications relevant to implants, devices, and cell-based therapies. Further development of these important technologies promises to enable new therapies, diagnostics, and revolutionize the management of patient care for many intractable diseases.
Keywords: Alginate; Biomaterials; Cell encapsulation; Devices; Diabetes; Fibrosis; Foreign body response; Hydrogel; Immunology; Immunomodulation; Implantation; Zwitterionic.
Copyright © 2019. Published by Elsevier B.V.
Conflict of interest statement
Disclosure
The authors of this manuscript have conflicts of interest to disclose as described by Advanced Drug Delivery Reviews. O.V. and A.J.V. are scientific founders of Sigilon Therapeutics.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
