

Can molecular stratification improve the treatment of inflammatory bowel disease?
- PMID: 31491469
- PMCID: PMC6902263
- DOI: 10.1016/j.phrs.2019.104442
Can molecular stratification improve the treatment of inflammatory bowel disease?
Abstract
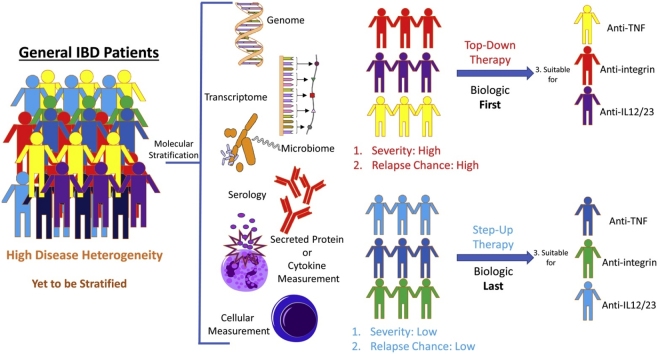
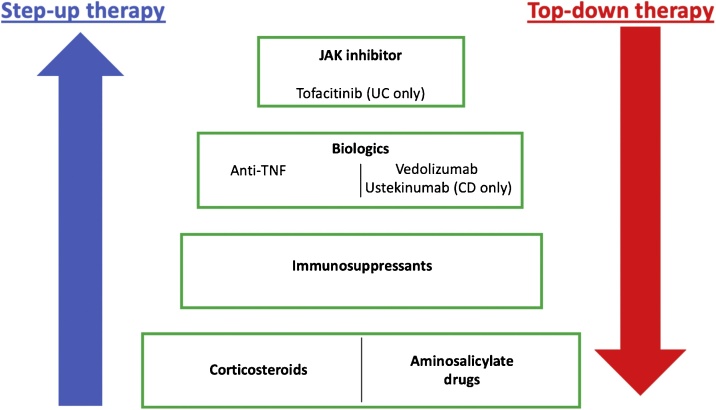
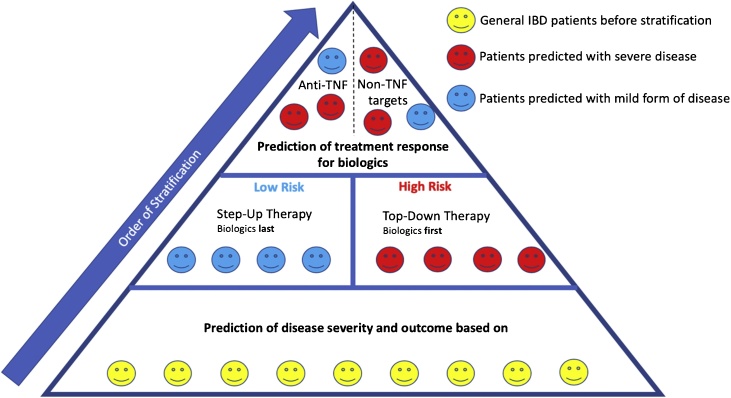
Inflammatory bowel disease (IBD) is a debilitating chronic inflammatory disease of the gastrointestinal (GI) tract. It affects more than 3.5 million people in the western world and places a huge financial burden on healthcare systems. IBD is highly heterogeneous; disease severity and outcomes in IBD are highly variable, and patients may experience episodes of relapse and remission. However, treatment often follows a step-up model whereby the patients start with anti-inflammatory agents (corticosteroids or immunosuppressants) and step-up to monoclonal anti-tumour necrosis factor-α (TNFα) antibodies and then other biologics if the initial drugs cannot control disease. Unfortunately, many patients do not respond to the costly biologics, and thus often still require gut-resective surgery, which decreases quality of life. In order to decrease rates of surgery and ineffective treatments, it is important to identify markers that accurately predict disease progression and treatment responses, to inform decisions about the best choice of therapeutics. Here we examine molecular approaches to patient stratification that aim to increase the effectiveness of treatments and potentially reduce healthcare costs. In the future, it may become possible to stratify patients based on their suitability for specific molecular-targeted therapeutic agents, and eventually use molecular stratification for personalised medicine in IBD.
Keywords: Anti-TNF; Biologics; CD; Crohn’s disease; Disease stratification; Faecal calprotectin; Genomics; Inflammatory bowel disease; Microbiomics; Molecular stratification; Precision medicine; Proteomics; Serological markers; Transcriptomics; Treatment response; UC; Ulcerative Colitis.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
