

Metabolic Unhealthiness Increases the Likelihood of Having Metabolic Syndrome Components in Normoweight Young Adults
- PMID: 31491867
- PMCID: PMC6765795
- DOI: 10.3390/ijerph16183258
Metabolic Unhealthiness Increases the Likelihood of Having Metabolic Syndrome Components in Normoweight Young Adults
Abstract
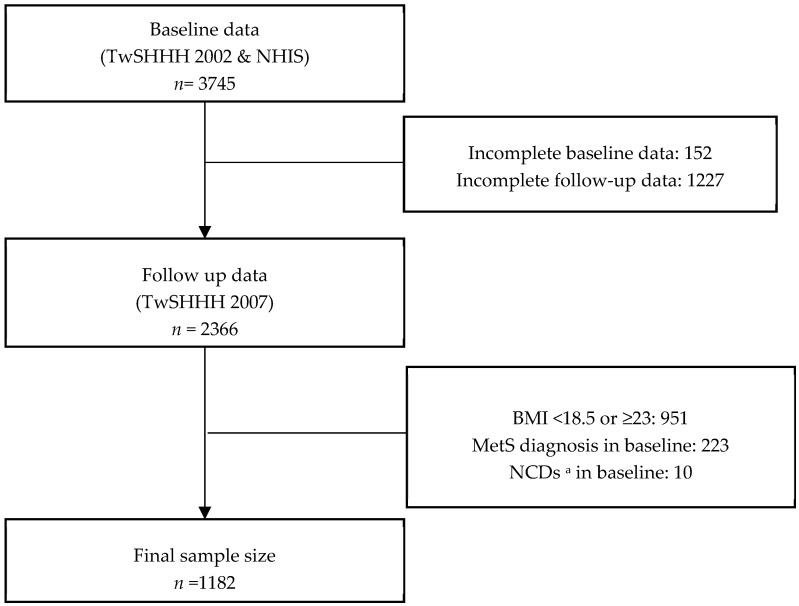
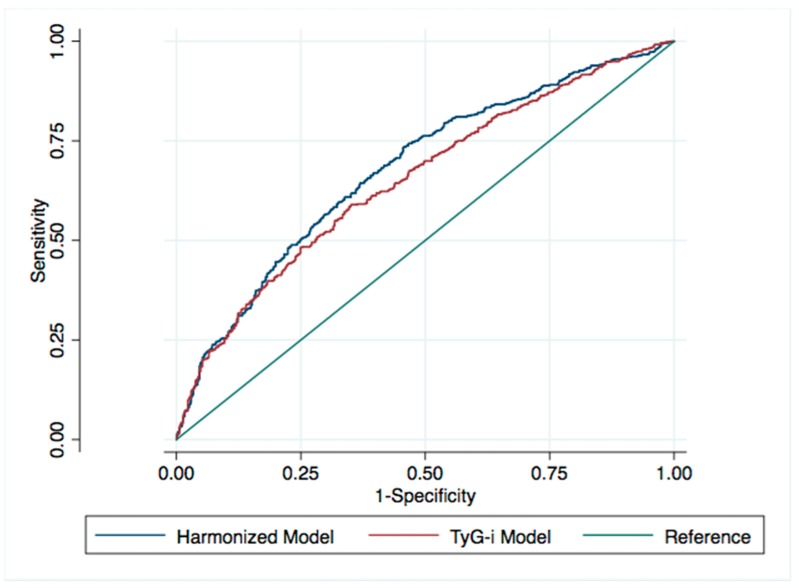
Findings on risk detection for having metabolic syndrome (MetS) components, each of which may individually increase the risk of disease and mortality, are limited in young adults. In this study, we aimed to calculate the likelihood of having ≥1 MetS component in normoweight young adults using two different metabolic health criteria. We recruited 1182 normoweight young adults from the Taiwan Survey on the Prevalence of Hypertension, Hyperglycemia, and Hyperlipidemia and the National Health Interview Survey (aged 16-45 years, 39% male, body mass index = 18.5-22.99, all without MetS) and followed them for 5 years. Metabolic health criteria were derived from the Harmonized criteria (unhealthy if showing abnormality in one or two MetS components) and the triglyceride-glucose index (TyG-i; unhealthy if TyG-i was in the >75th percentile). Odds ratio (OR) and 95% confidence interval (CI) estimations for having ≥1 MetS component and for having each MetS component in 5 years were assessed using multivariable-adjusted logistic regression. We observed a significantly increased likelihood of the presence of ≥1 MetS component in the unhealthy group by using the Harmonized criteria and TyG-i (adjusted OR (aOR); 95%CI: 2.67; 2.04-3.49 and 2.1; 1.57-2.82, respectively). The areas under the receiver-operating characteristics curves were 0.679 and 0.652 for the final models using Harmonized and TyG-i criteria, respectively. These findings support the recommendation of treating any metabolic component abnormality, even in young adults without a MetS diagnosis.
Keywords: cardiovascular disease prevention; cohort; insulin resistance; metabolic health; metabolic syndrome; national survey; young adult.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Folsom A.R., Shah A.M., Lutsey P.L., Roetker N.S., Alonso A., Avery C.L., Miedema M.D., Konety S., Chang P.P., Solomon S.D. American Heart Association’s Life’s Simple 7: Avoiding Heart Failure and Preserving Cardiac Structure and Function. Am. J. Med. 2015;128:970–976. doi: 10.1016/j.amjmed.2015.03.027. - DOI - PMC - PubMed
-
- Ng M., Fleming T., Robinson M., Thomson B., Graetz N., Margono C., Mullany E.C., Biryukov S., Abbafati C., Abera S.F., et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi: 10.1016/S0140-6736(14)60460-8. - DOI - PMC - PubMed
-
- Alberti K.G.M.M., Eckel R.H., Grundy S.M., Zimmet P.Z., Cleeman J.I., Donato K.A., Fruchart J.C., James W.P.T., Loria C.M., Smith S.C. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; National heart, lung, and blood institute; American heart association; World heart federation; International. Circulation. 2009;120:1640–1645. doi: 10.1161/CIRCULATIONAHA.109.192644. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
