

Indirect Calorimetry in Clinical Practice
- PMID: 31491883
- PMCID: PMC6780066
- DOI: 10.3390/jcm8091387
Indirect Calorimetry in Clinical Practice
Abstract
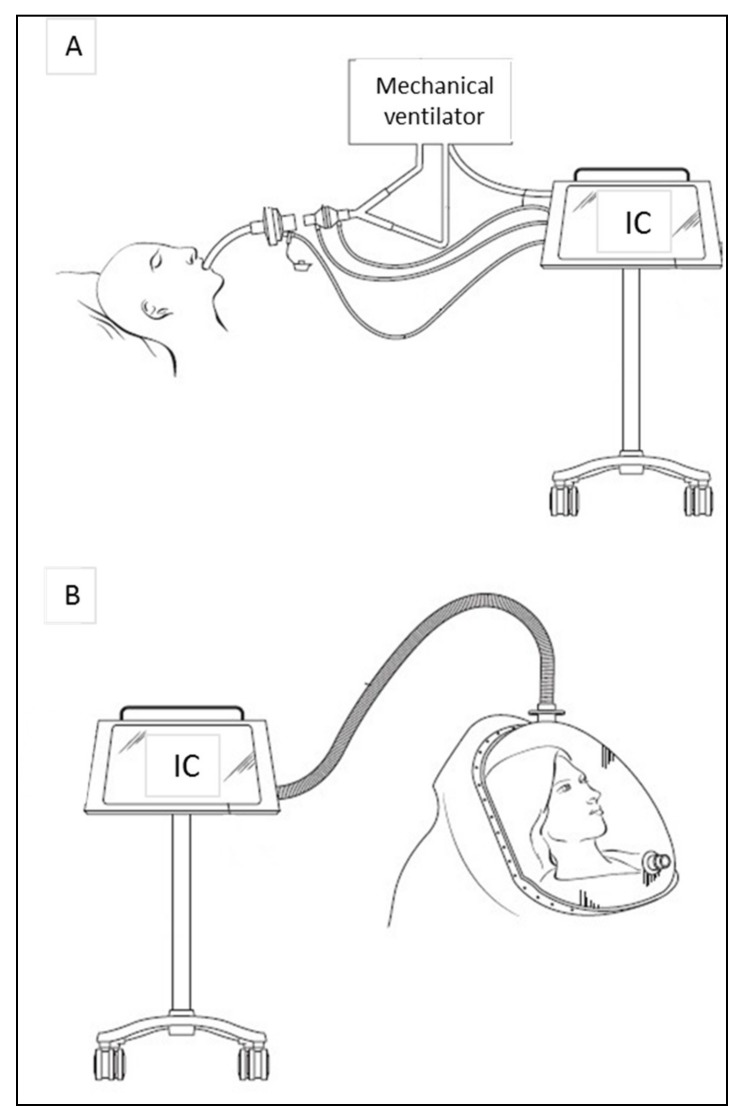
Indirect calorimetry (IC) is considered as the gold standard to determine energy expenditure, by measuring pulmonary gas exchanges. It is a non-invasive technique that allows clinicians to personalize the prescription of nutrition support to the metabolic needs and promote a better clinical outcome. Recent technical developments allow accurate and easy IC measurements in spontaneously breathing patients as well as in those on mechanical ventilation. The implementation of IC in clinical routine should be promoted in order to optimize the cost-benefit balance of nutrition therapy. This review aims at summarizing the latest innovations of IC as well as the clinical indications, benefits, and limitations.
Keywords: indirect calorimeter; indirect calorimetry; nutrition therapy; resting energy expenditure.
Conflict of interest statement
CP received financial support as an unrestricted academic research grant from public institutions (Geneva University Hospital) and the Foundation Nutrition 2000 Plus. CP received financial support as research grants and an unrestricted academic research grant, as well as an unrestricted research grant and consulting fees, from Abbott, Baxter, B. Braun, Cosmed, Fresenius-Kabi, Nestle Medical Nutrition, Novartis, Nutricia-Numico, Pfizer, and Solvay, outside the submitted work. M.M.B. received research grants and public academic research grants, unrestricted research grand from Fresenius Kabi International, consulting fees from Fresenius Kabi International, and honoraria for lectures for Fresenius Kabi, Nestle. The other authors declare that they have no conflict of interest related to the current work. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Singer P., Anbar R., Cohen J., Shapiro H., Shalita-Chesner M., Lev S., Grozovski E., Theilla M., Frishman S., Madar Z. The tight calorie control study (TICACOS), a prospective, randomized, controlled pilot study of nutritional support in critically ill patients. Intensiv. Care Med. 2011;37:601–609. doi: 10.1007/s00134-011-2146-z. - DOI - PubMed
-
- Heidegger C.P., Berger M.M., Graf S., Zingg W., Darmon P., Costanza M.C., Thibault R., Pichard C. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: A randomised controlled clinical trial. Lancet. 2013;381:385–393. doi: 10.1016/S0140-6736(12)61351-8. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
