

Antifibrotic therapy for idiopathic pulmonary fibrosis: time to treat
- PMID: 31492155
- PMCID: PMC6731623
- DOI: 10.1186/s12931-019-1161-4
Antifibrotic therapy for idiopathic pulmonary fibrosis: time to treat
Abstract
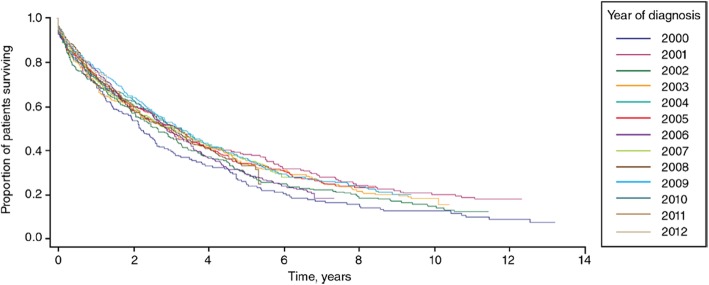
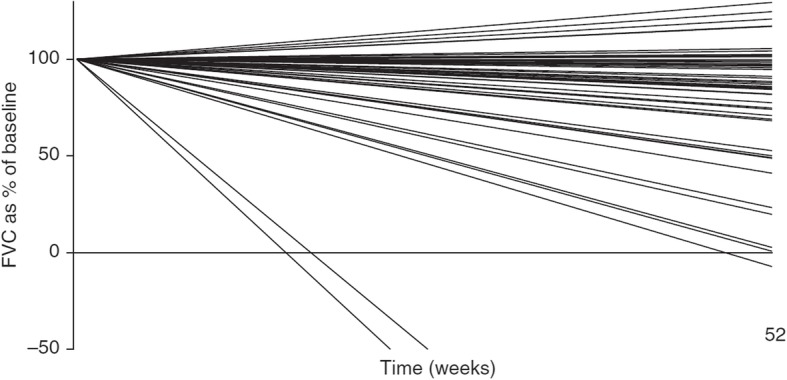
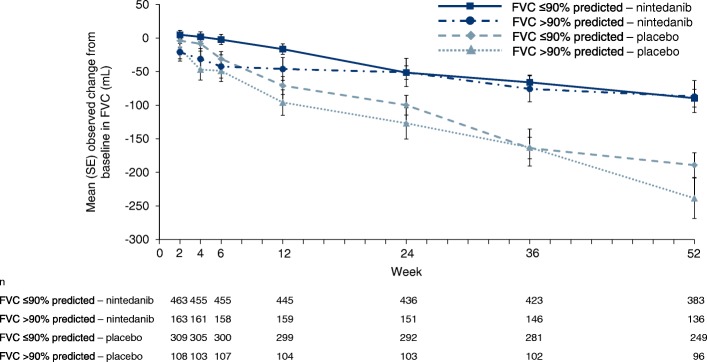
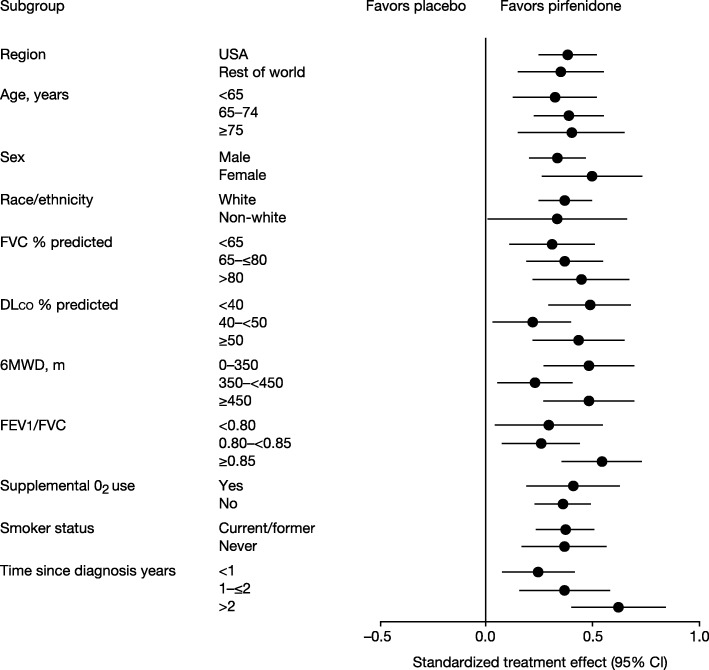
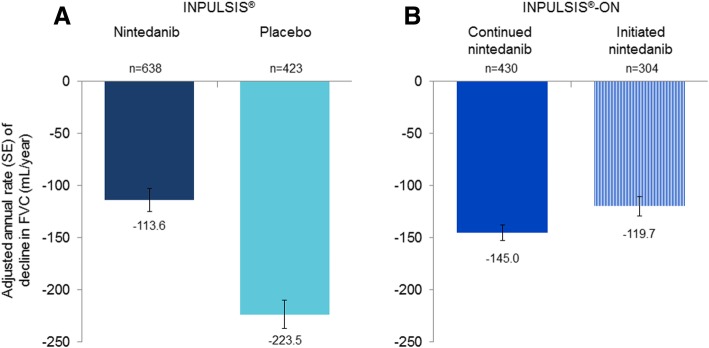
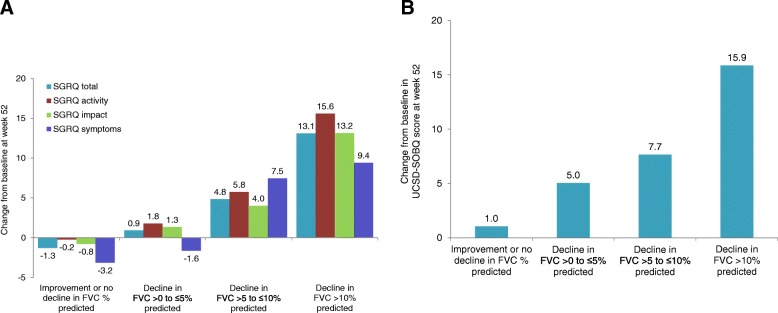
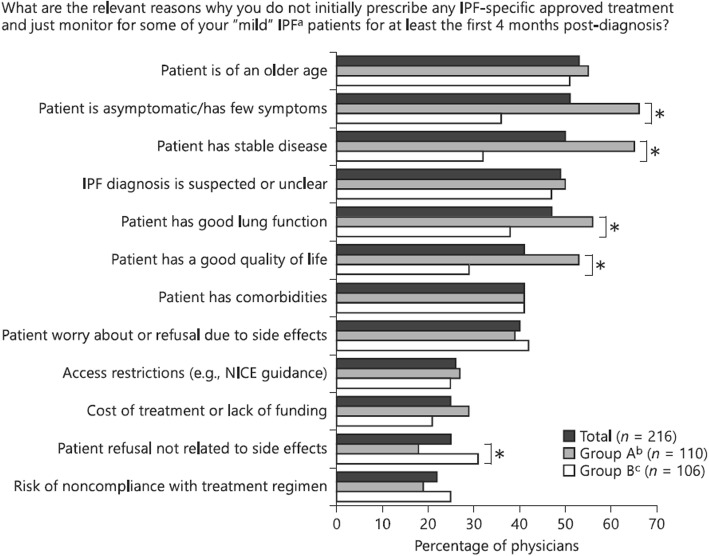
Idiopathic pulmonary fibrosis (IPF) is a progressive disease with a dismal prognosis. The average life expectancy of untreated patients with IPF is only 3 to 4 years. Decline in forced vital capacity (FVC) in patients with IPF appears to be almost linear, with patients with well-preserved FVC at baseline experiencing the same rate of decline in FVC as patients with more advanced disease. Two antifibrotic therapies have been approved for the treatment of IPF: nintedanib and pirfenidone. These drugs slow decline in lung function and reduce the risk of acute respiratory deteriorations, which are associated with very high morbidity and mortality. Individual clinical trials have not been powered to show reductions in mortality, but analyses of pooled data from clinical trials, as well as observational studies, suggest that antifibrotic therapies improve life expectancy. Despite this, many individuals with IPF remain untreated. In many cases, this is because the physician perceives that the disease is stable and so does not warrant therapy, or has concerns over the potential side-effects of antifibrotic drugs. There remains a need to educate pulmonologists that IPF is a progressive, irreversible and fatal disease and that prompt treatment is critical to preserving patients' lung function and improving outcomes. Most individuals can tolerate antifibrotic therapy, and dose adjustment has been shown to be effective at reducing side effects without compromising efficacy. In addition to anti-fibrotic therapies, individuals with IPF benefit from a holistic approach to their care that includes symptom management and supportive care tailored to the needs of the individual. An animation illustrating the themes covered in this article will be available at: http://www.usscicomms.com/respiratory/maher/treatment-of-IPF .
Keywords: Interstitial lung disease; Mortality; Nintedanib; Pirfenidone; Therapeutics; Treatment.
Conflict of interest statement
Outside the submitted work, TMM reports receiving grant funding to his institution and personal fees for service on a clinical trial advisory board from GlaxoSmithKline; personal fees from Boehringer Ingelheim, InterMune/Roche, Sanofi Aventis, AstraZeneca, Biogen Idec, Cipla, Prometic and Sanumed; research fees to his institution; personal fees and non-financial support from UCB; he holds stock options in Apellis. Outside the submitted work, MES reports grants from Boehringer Ingelheim, Novartis, Roche and the National Institutes of Health, and personal fees from Boehringer Ingelheim.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
