

Congenital anomalies and associated risk factors in a Saudi population: a cohort study from pregnancy to age 2 years
- PMID: 31492776
- PMCID: PMC6731804
- DOI: 10.1136/bmjopen-2018-026351
Congenital anomalies and associated risk factors in a Saudi population: a cohort study from pregnancy to age 2 years
Abstract
Objective: To assess the three key issues for congenital anomalies (CAs) prevention and care, namely, CA prevalence, risk factor prevalence and survival, in a longitudinal cohort in Riyadh, Saudi Arabia.
Setting: Tertiary care centre, Riyadh, Saudi Arabia.
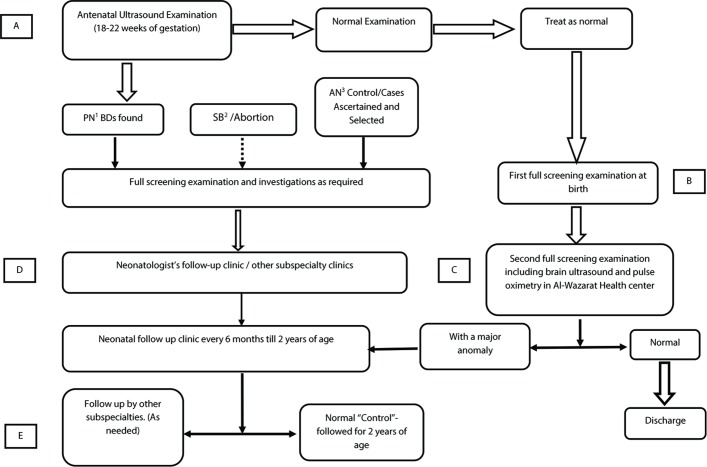
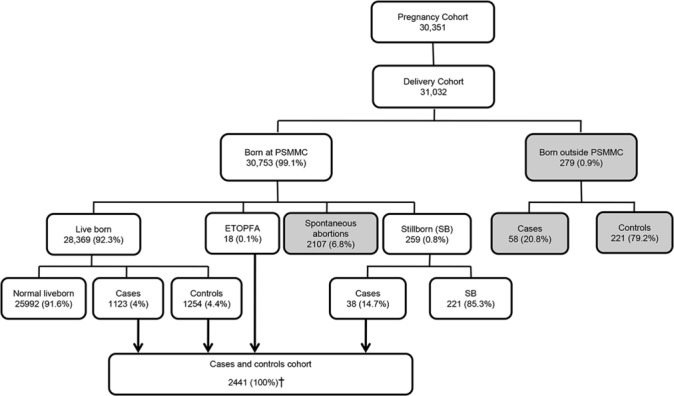
Participants: Saudi women enrolled during pregnancy over 3 years and their 28 646 eligible pregnancy outcomes (births, stillbirths and elective terminations of pregnancy for foetal anomalies). The nested case-control study evaluated the CA risk factor profile of the underlying cohort. All CA cases (1179) and unaffected controls (1262) were followed through age 2 years. Referred mothers because of foetal anomaly and mothers who delivered outside the study centre and their pregnancy outcome were excluded.
Primary outcome measures: Prevalence and pattern of major CAs, frequency of CA-related risk factors and survival through age 2 years.
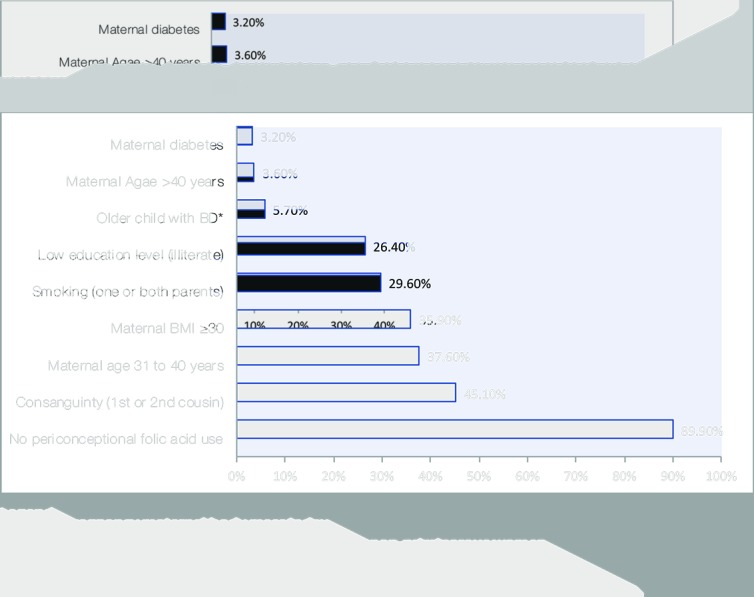
Results: The birth prevalence of CAs was 412/10 000 births (95% CI 388.6 to 434.9), driven mainly by congenital heart disease (148 per 10 000) (95% CI 134 to 162), renal malformations (113, 95% CI 110 to 125), neural tube defects (19, 95% CI 25.3 to 38.3) and chromosomal anomalies (27, 95% CI 21 to 33). In this study, the burden of potentially modifiable risk factors included high rates of diabetes (7.3%, OR 1.98, 95% CI 1.04 to 2.12), maternal age >40 years (7.0%, OR 2.1, 95% CI 1.35 to 3.3), consanguinity (54.5%, OR 1.5, 95% CI 1.28 to 1.81). The mortality for live births with CAs at 2 years of age was 15.8%.
Conclusions: This study documented specific opportunities to improve primary prevention and care. Specifically, folic acid fortification (the neural tube defect prevalence was >3 times that theoretically achievable by optimal fortification), preconception diabetes screening and consanguinity-related counselling could have significant and broad health benefits in this cohort and arguably in the larger Saudi population.
Keywords: congenital anomalies; outcome; prevalence; prevention; risk factors.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization Sixty -Third World health assembly. Ca report by the Secretariat, A63/10. Geneva, Switzerland: World Health Organization, 2010.
-
- World Health Organization Global health Observatory (GHO) data. Under-five mortality, 2016. Available: http://www.who.int/gho/child_health/mortality/mortality_under_five_text/en/ [Accessed 12 Dec 2017].
-
- Christianson AL, Howson CP, Modell B. Global report on CA: the hidden toll of dying and disabled children. White Plains (NY): March of Dimes Defects Foundation, 2006.
-
- Wang Y, Hu J, Druschel CM, et al. Twenty-five–year survival of children with birth defects in New York state: a population-based study. Birth Defects Research;201:995–1003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases