

Validation and assessment of an antibiotic-based, aseptic decontamination manufacturing protocol for therapeutic, vacuum-dried human amniotic membrane
- PMID: 31492886
- PMCID: PMC6731261
- DOI: 10.1038/s41598-019-49314-7
Validation and assessment of an antibiotic-based, aseptic decontamination manufacturing protocol for therapeutic, vacuum-dried human amniotic membrane
Abstract
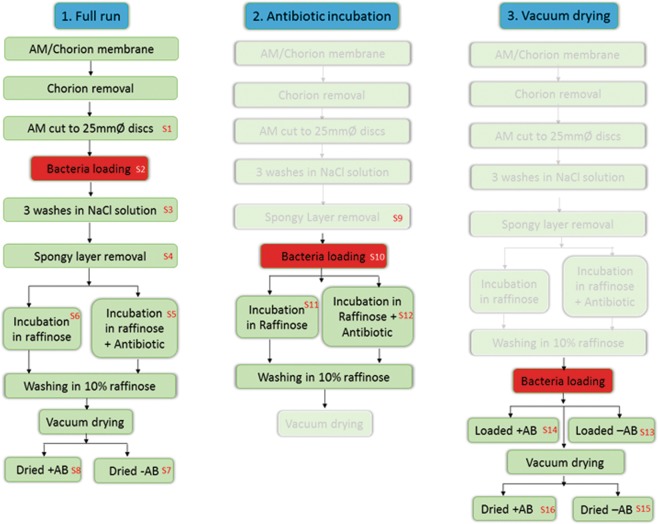
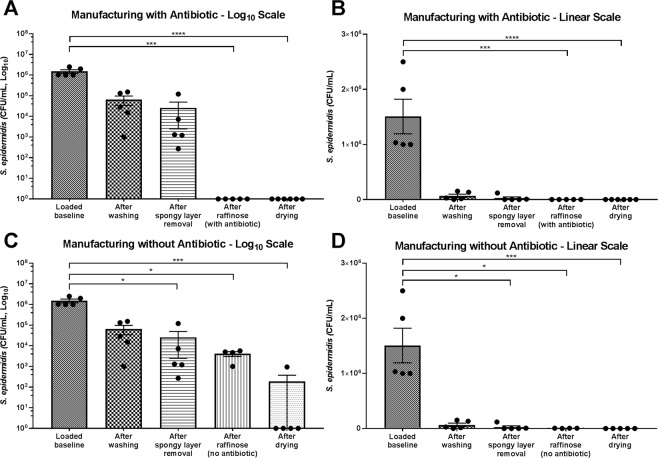
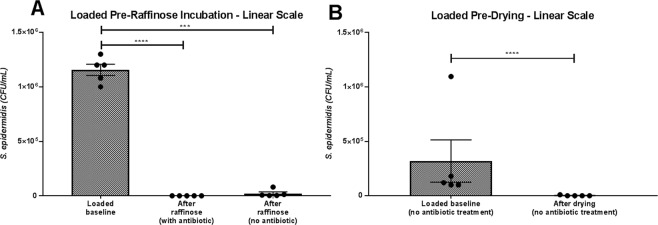
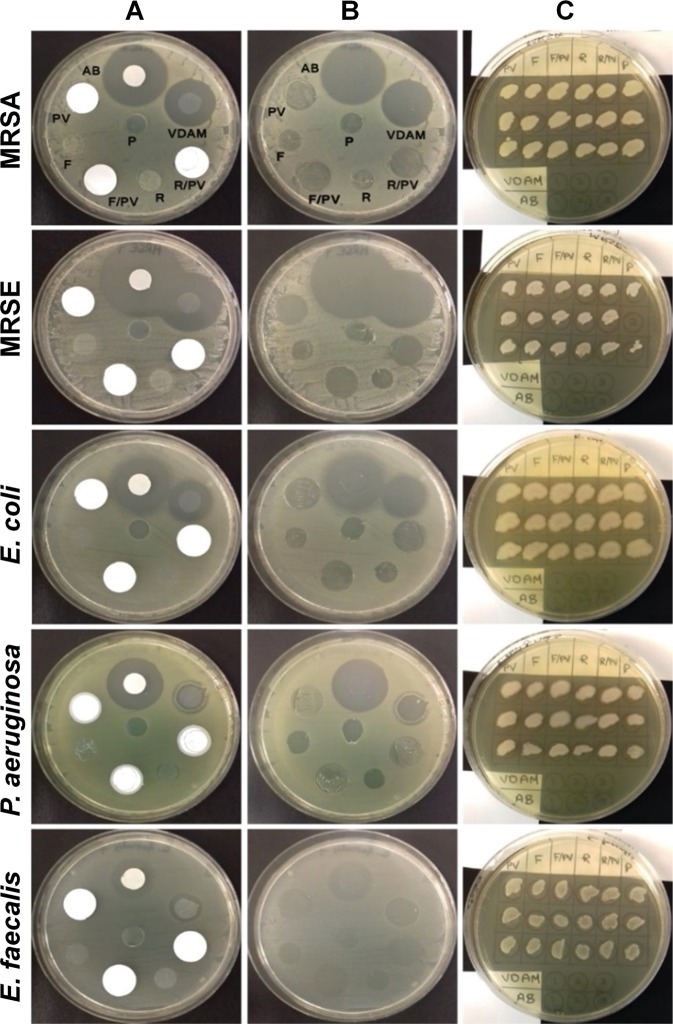
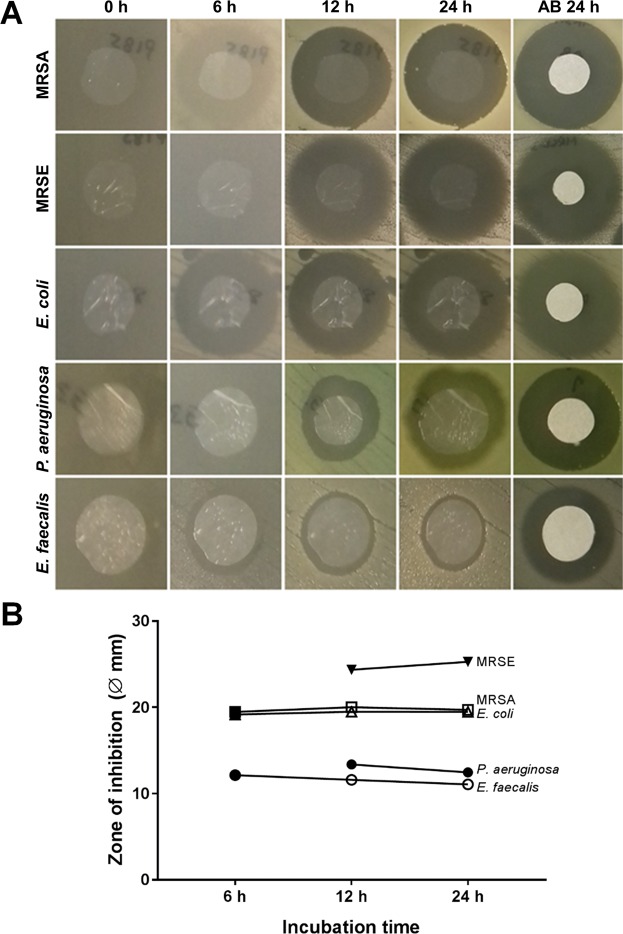
Amniotic membrane (AM) is used to treat a range of ophthalmic indications but must be presented in a non-contaminated state. AM from elective caesarean sections contains natural microbial contamination, requiring removal during processing protocols. The aim of this study was to assess the ability of antibiotic decontamination of AM, during processing by innovative low-temperature vacuum-drying. Bioburden of caesarean section AM was assessed, and found to be present in low levels. Subsequently, the process for producing vacuum-dried AM (VDAM) was assessed for decontamination ability, by artificially loading with Staphylococcus epidermidis at different stages of processing. The protocol was highly efficient at removing bioburden introduced at any stage of processing, with antibiotic treatment and drying the most efficacious steps. The antibacterial activity of non-antibiotic treated AM compared to VDAM was evaluated using minimum inhibitory/biocidal concentrations (MIC/MBC), and disc diffusion assays against Meticillin-resistant Staphylococcus aureus, Meticillin-resistant S. epidermidis, Escherichia coli, Pseudomonas aeruginosa and Enterococcus faecalis. Antibacterial activity without antibiotic was low, confirmed by high MIC/MBC, and a no inhibition on agar lawns. However, VDAM with antibiotic demonstrated effective antibacterial capacity against all bacteria. Therefore, antibiotic decontamination is a reliable method for sterilisation of AM and the resultant antibiotic reservoir is effective against gram-positive and -negative bacteria.
Conflict of interest statement
Dr. Hopkinson and Dr. Allen own shares in NuVision Biotherapies. Dr. Hopkinson, Dr. Britchford and Mr. McIntosh were partially employed by NuVision Biotherapies whilst this study took place. Dr. Sidney, Mr. Ashraf and Prof. Bayston declare no potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
