

Adhesive and non-adhesive internal hernia: clinical relevance and multi-detector CT images
- PMID: 31492915
- PMCID: PMC6731239
- DOI: 10.1038/s41598-019-48241-x
Adhesive and non-adhesive internal hernia: clinical relevance and multi-detector CT images
Abstract
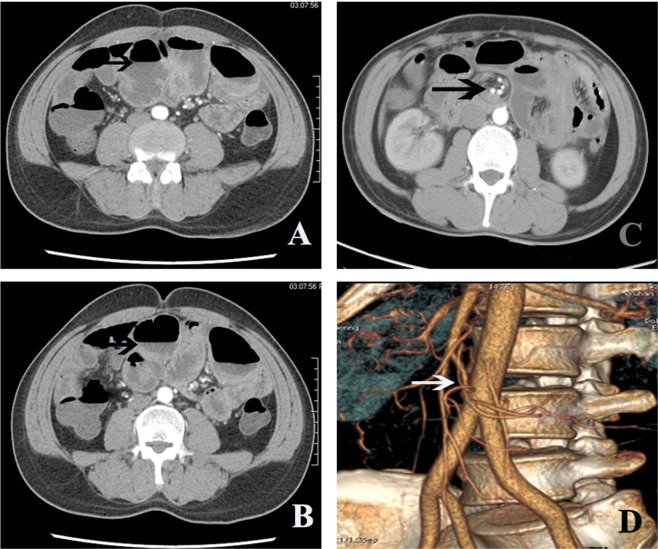
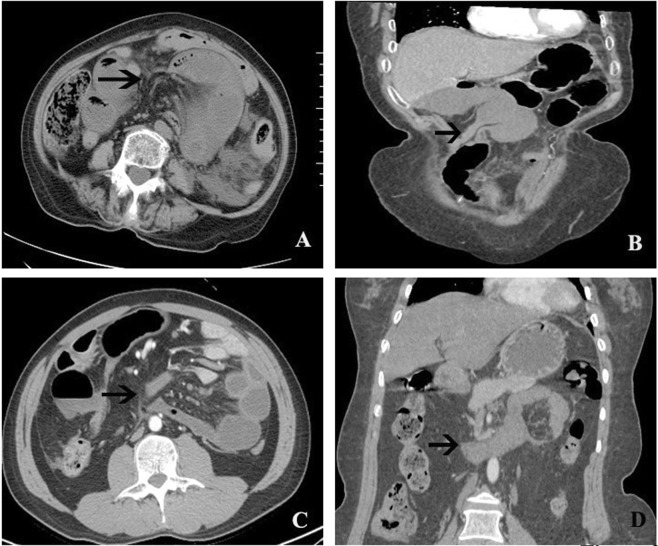
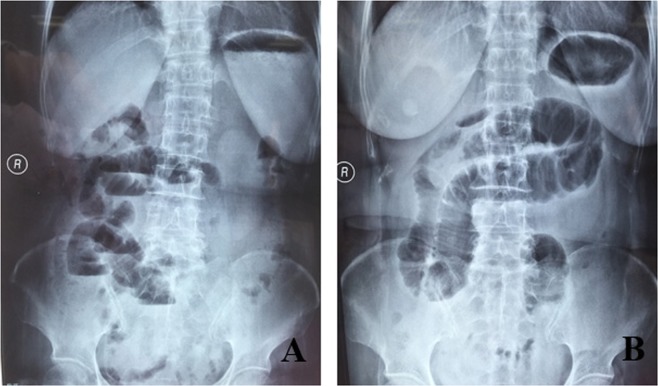
Internal hernia (IH)-related surgical acute abdomen is not well understood because of the rarity of cases and underdiagnosis. This study was performed to further understand the clinicopathological features and multi-detector computed tomography (MDCT) findings of IH in cases confirmed by surgery. In all, 51 patients with a definite diagnosis of IH confirmed during surgical exploration from Feb. 2012 to Feb. 2018 in our hospital were included in this research. Medical records, including MDCT images and intra-operative findings, were collected retrospectively. In all, 39 and 12 cases were categorized as adhesive IH (76.5%) and non-adhesive IH (23.5%), respectively. Among the patients with adhesive IH, 73% had a history of abdominal or pelvic surgery. Additionally, the mesentery was the most common component of adhesive bands (64.1%). Congenital peritoneal abnormalities and gastrointestinal reconstruction were the main causes of non-adhesive IH.As a specific sign, the fat notch sign was much more common in adhesive IH than in non-adhesive IH (P = 0.023). Bowel wall thickening (P = 0.041), abnormal bowel wall enhancement (P = 0.006) and twisted bowels with the vessel swirl sign (P = 0.004) were indicators of bowel necrosis. Among all of the cases of IH, 34 (66.7%) were complicated by bowel necrosis, and 1 patient died. In conclusion, non-adhesive IH has different clinicopathological features and MDCT findings from those of adhesive IH. MDCT is a useful tool with high sensitivity for confirming IH and may help to guide the early treatment of IH.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Adhesive internal hernia: multidetector CT findings and clinical relevance.Clin Radiol. 2018 Feb;73(2):218.e1-218.e7. doi: 10.1016/j.crad.2017.08.007. Epub 2017 Dec 15. Clin Radiol. 2018. PMID: 29102485
-
Multidetector Computed Tomography Findings of Adhesive Internal Hernias.J Comput Assist Tomogr. 2020 Jan/Feb;44(1):131-137. doi: 10.1097/RCT.0000000000000955. J Comput Assist Tomogr. 2020. PMID: 31939894
-
Internal hernia: computed tomography diagnosis and differentiation from adhesive small bowel obstruction.J Chin Med Assoc. 2005 Jan;68(1):21-8. doi: 10.1016/S1726-4901(09)70127-3. J Chin Med Assoc. 2005. PMID: 15742859
-
Internal hernias after abdominal surgeries: MDCT features.Abdom Imaging. 2011 Aug;36(4):349-62. doi: 10.1007/s00261-010-9627-3. Abdom Imaging. 2011. PMID: 20512488 Review.
-
Adhesive Small Bowel Obstruction: Predictive Radiology to Improve Patient Management.Radiology. 2020 Sep;296(3):480-492. doi: 10.1148/radiol.2020192234. Epub 2020 Jul 21. Radiology. 2020. PMID: 32692296 Review.
Cited by
-
Congenital Dual Internal Hernias Causing Small Bowel Obstruction in a Man with no Prior Surgical History: A Report of a Very Rare Case.Am J Case Rep. 2021 Jul 13;22:e932132. doi: 10.12659/AJCR.932132. Am J Case Rep. 2021. PMID: 34255765 Free PMC article.
-
Cecal bascule presenting as internal hernia.J Surg Case Rep. 2024 May 31;2024(5):rjae366. doi: 10.1093/jscr/rjae366. eCollection 2024 May. J Surg Case Rep. 2024. PMID: 38826857 Free PMC article.
-
Radiomics-based machine learning model for diagnosing internal abdominal hernias: a retrospective study.Sci Rep. 2025 May 22;15(1):17803. doi: 10.1038/s41598-025-02534-6. Sci Rep. 2025. PMID: 40404730 Free PMC article.
-
Internal Hernia Through a Mesenteric Defect Presenting As Midgut Volvulus: A Rare and Intriguing Coexistence.Cureus. 2025 Jun 5;17(6):e85426. doi: 10.7759/cureus.85426. eCollection 2025 Jun. Cureus. 2025. PMID: 40621280 Free PMC article.
-
Small bowel obstruction and strangulation secondary to an adhesive internal hernia post ESWL for right ureteral calculi: a case report and review of literature.BMC Gastroenterol. 2021 Apr 17;21(1):176. doi: 10.1186/s12876-021-01760-2. BMC Gastroenterol. 2021. PMID: 33865311 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
