

A Pilot Randomized Controlled Trial of Outcomes Associated with Parent-Nurse Controlled Analgesia vs. Continuous Opioid Infusion in the Neonatal Intensive Care Unit
- PMID: 31494028
- PMCID: PMC6980456
- DOI: 10.1016/j.pmn.2019.08.002
A Pilot Randomized Controlled Trial of Outcomes Associated with Parent-Nurse Controlled Analgesia vs. Continuous Opioid Infusion in the Neonatal Intensive Care Unit
Abstract
Purpose: Prospectively compare parent/nurse controlled analgesia (PNCA) to continuous opioid infusion (COI) in the post-operative neonatal intensive care unit (NICU) population.
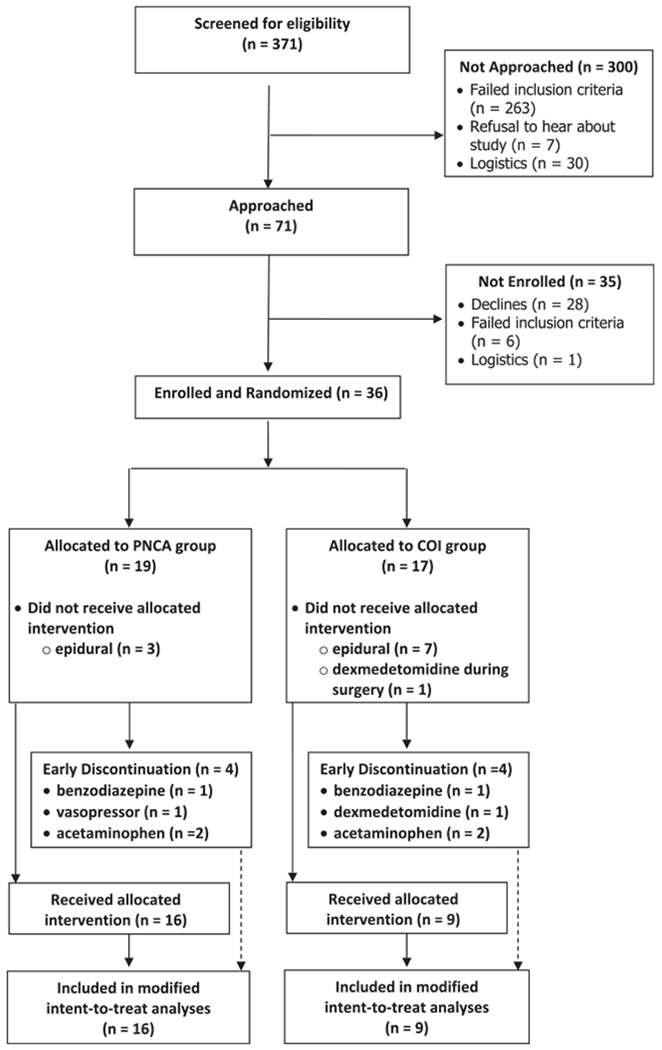
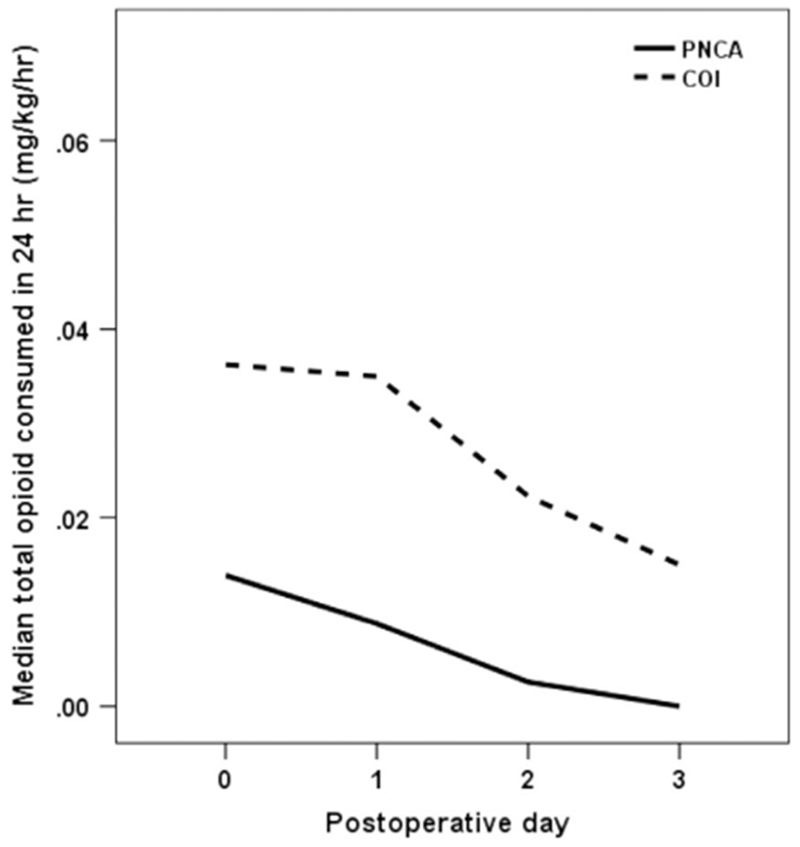
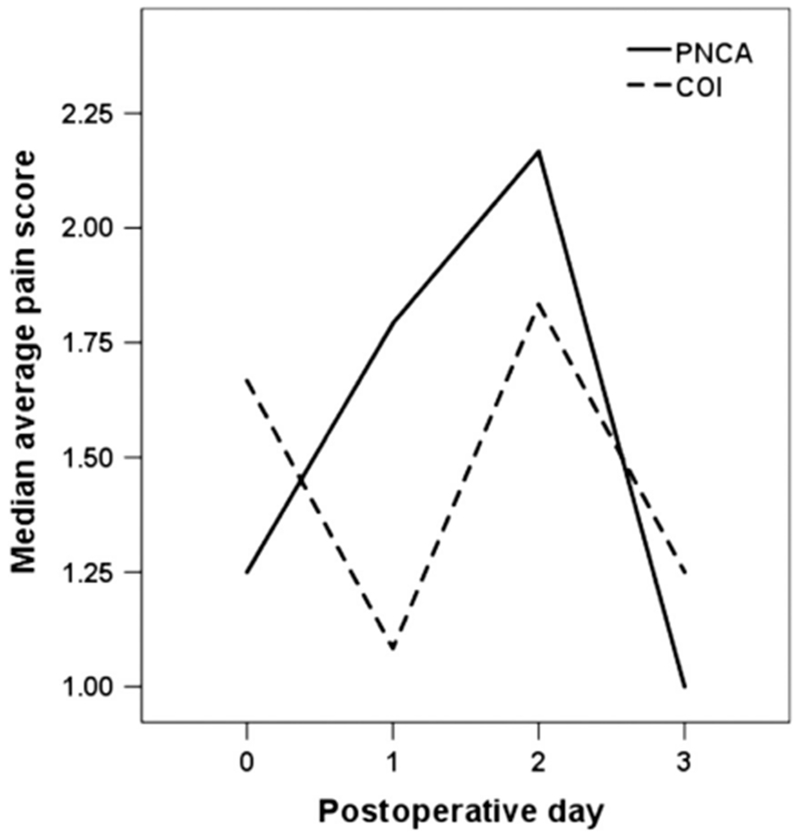
Design/methods: A randomized controlled trial compared neonates treated with morphine PNCA to those treated with morphine COI. The primary outcome was average opioid consumption up to 3 post-operative days. Secondary outcomes included 1) pain intensity, 2) adverse events that may be directly related to opioid consumption, and 3) parent and nurse satisfaction.
Results: The sample consisted of 25 post-operative neonates and young infants randomized to either morphine PNCA (n = 16) or COI (n = 9). Groups differed significantly on daily opioid consumption, with the PNCA group receiving significantly less opioid (P = .02). Groups did not differ on average pain score or frequency of adverse events (P values > .05). Parents in both groups were satisfied with their infant's pain management and parents in the PNCA group were slightly more satisfied with their level of involvement (P = .03). Groups did not differ in nursing satisfaction.
Conclusions: PNCA may be an effective alternative to COI for pain management in the NICU population. This method may also substantially reduce opioid consumption, provide more individualized care, and improve parent satisfaction with their level of participation.
Clinical implications: Patients in the NICU represent one of our most vulnerable patient populations. As nurses strive to provide safe and effective pain management, results of this study suggest PNCA may allow nurses to maintain their patients' comfort while providing less opioid and potentially improving parental perception of involvement.
Study type: Treatment study.
Level of evidence: I.
Trial registration: ClinicalTrials.gov NCT00743730.
Copyright © 2020 American Society for Pain Management Nursing. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ahn Y, Kang H, & Shin E (2005). Pain assessment using CRIES, FLACC and PIPP in high-risk infants. Taehan Kanho Hakhoe Chi, 35(7), 1401–1409. - PubMed
-
- Anand KJ, & Hickey PR (1987). Pain and its effects in the human neonate and fetus. The New England Journal of Medicine, 317(21),1321–1329. - PubMed
-
- Anghelescu DL, Kaddoum RN, Oakes LL, Windsor KB, Faughnan LG, & Burgoyne LL (2011). An update: The safety of patient-controlled analgesia by proxy for pain management in pediatric oncology: 2004 to 2010. Anesthesia and Analgesia, 113(6), 1525–1526. - PubMed
-
- Bell GC, Crews KR, Wilkinson MR, Haidar CE, Hicks JK, Baker DK, Kornegay NM, Yang W, Cross SJ, Howard SC, Freimuth RR, Evans WE, Broeckel U, Relling MV, & Hoffman JM (2014). Development and use of active clinical decision support for preemptive pharmacogenomics. Journal of the American Medical Informatics Association: JAMIA, 21 (e1), e93–e99. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
